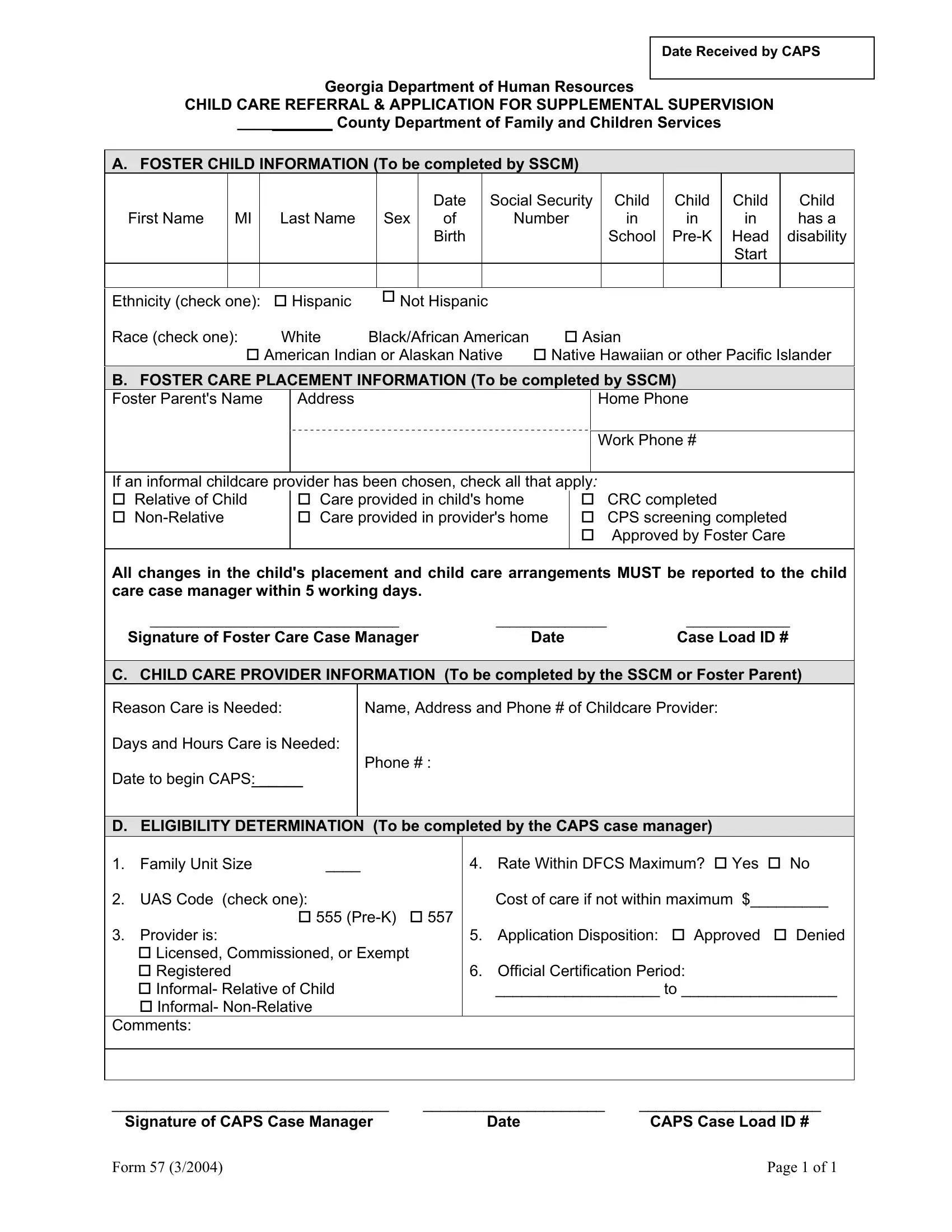
In Georgia, a crucial document known as Form 57 serves as a bridge for foster children and their caregivers to access supplemental supervision and childcare services. Managed by the Georgia Department of Human Resources, specifically through the Childcare and Parent Services (CAPS) division, this form encompasses a comprehensive process. It begins with the detailed capture of foster child information, including personal identifiers, educational status, and any disability notes, highlighting the state's commitment to accommodating diverse needs. Additionally, it collects foster care placement details, fostering transparency between foster parents and childcare case managers about the living and care arrangements of the child. The form facilitates a check on informal childcare providers, ensuring they meet specified criteria such as relation to the child and completion of required screenings. Moreover, it guides through the eligibility criteria set by the CAPS case manager, encompassing family unit size, codes associated with the care needed, and the financial aspects of the care provided. This form not only ensures that children in foster care receive proper supervision and care but also underscores the structured approach Georgia takes to fulfill these needs, including a focus on financial feasibility and compliance with state guidelines.
| Question | Answer |
|---|---|
| Form Name | Georgia Form 57 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Islander, SSCM, childcare, CPS |
Date Received by CAPS
Georgia Department of Human Resources
CHILD CARE REFERRAL & APPLICATION FOR SUPPLEMENTAL SUPERVISION
___________ County Department of Family and Children Services
A. FOSTER CHILD INFORMATION (To be completed by SSCM)
First Name MI Last Name Sex
Date |
Social Security |
Child |
Child |
of |
Number |
in |
in |
Birth |
|
School |
|
|
|
|
|
Child
in
Head
Start
Child has a disability
Ethnicity (check one): |
Hispanic |
Not Hispanic |
|
Race (check one): |
White |
Black/African American |
Asian |
|
American Indian or Alaskan Native |
Native Hawaiian or other Pacific Islander |
|
B. FOSTER CARE PLACEMENT INFORMATION (To be completed by SSCM)
Foster Parent's Name
Address
Home Phone
|
|
|
Work Phone # |
|
|
|
|
If an informal childcare provider has been chosen, check all that apply: |
|
||
Relative of Child |
Care provided in child's home |
|
CRC completed |
Care provided in provider's home |
|
CPS screening completed |
|
|
|
|
Approved by Foster Care |
|
|
|
|
All changes in the child's placement and child care arrangements MUST be reported to the child care case manager within 5 working days.
____________________________________ |
________________ |
_______________ |
Signature of Foster Care Case Manager |
Date |
Case Load ID # |
C. CHILD CARE PROVIDER INFORMATION (To be completed by the SSCM or Foster Parent)
Reason Care is Needed:
Days and Hours Care is Needed:
Date to begin CAPS: _____
Name, Address and Phone # of Childcare Provider:
Phone # :
D. ELIGIBILITY DETERMINATION (To be completed by the CAPS case manager)
1. |
Family Unit Size |
____ |
|
4. |
Rate Within DFCS Maximum? |
Yes |
No |
|
2. |
UAS Code (check one): |
|
|
|
Cost of care if not within maximum $_________ |
|||
|
|
555 |
557 |
|
|
|
|
|
3. |
Provider is: |
|
|
5. |
Application Disposition: |
Approved |
Denied |
|
|
Licensed, Commissioned, or Exempt |
|
|
|
|
|
|
|
|
Registered |
|
|
6. |
Official Certification Period: |
|
|
|
|
Informal- Relative of Child |
|
|
___________________ to __________________ |
||||
|
Informal- |
|
|
|
|
|
|
|
Comments:
________________________________ |
_____________________ |
_____________________ |
Signature of CAPS Case Manager |
Date |
CAPS Case Load ID # |
Form 57 (3/2004) |
Page 1 of 1 |