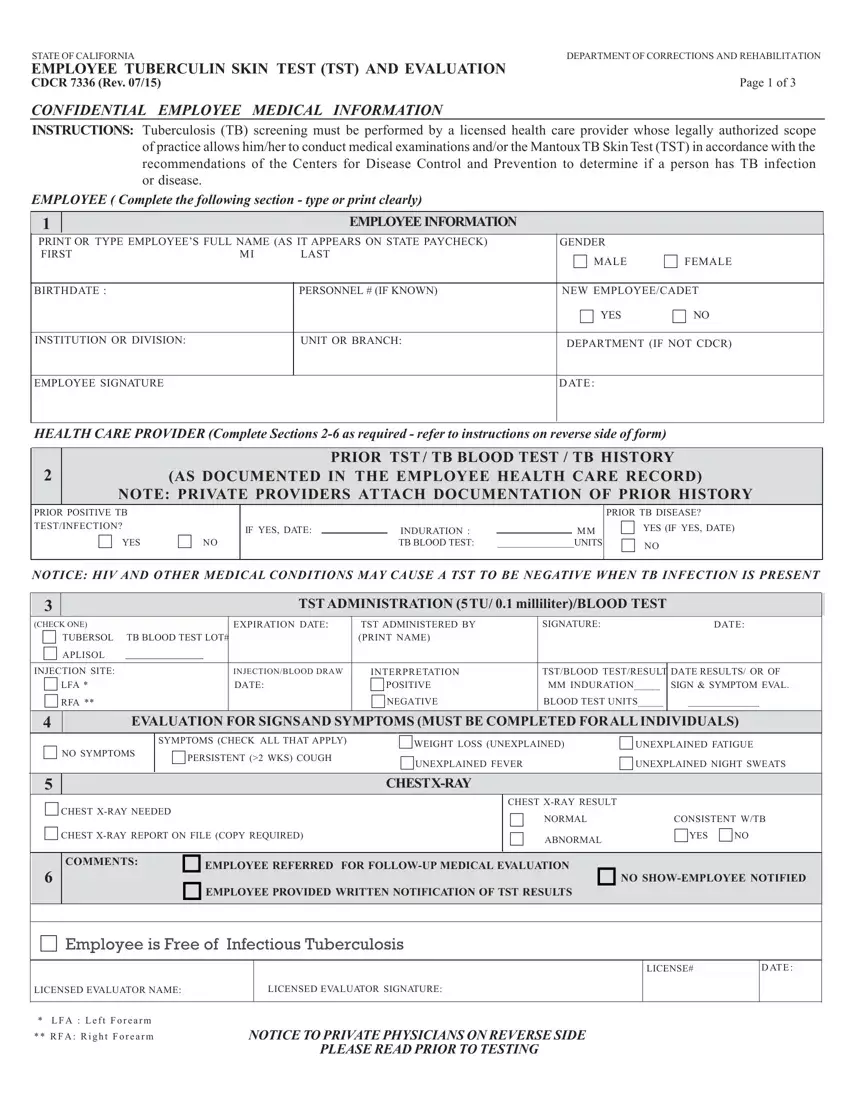
The CDCR 7336 form, revised in July 2015, serves as a critical tool in the health and safety protocols within the State of California Department of Corrections and Rehabilitation (CDCR), focusing on the prevention and control of Tuberculosis (TB) among its employees. This comprehensive document facilitates the screening and evaluation process by licensed healthcare providers for TB, adhering to the recommendations set forth by the Centers for Disease Control and Prevention. It encompasses detailed sections requiring personal and medical information from employees, instructions on prior TB test documentation, the administration and interpretation of the Tuberculin Skin Test (TST) or TB blood tests, evaluation for TB symptoms, the necessity for chest x-rays based on test results, and final assessment notes by the evaluator. The form prioritizes confidentiality while ensuring that all CDCR employees undergo an initial, annual, and medically necessary TB screening, encapsulating the process from employee personal data collection to the detailed reporting of the test and evaluation results. Moreover, it includes specific notices to private physicians regarding the medical information confidentiality required by the California Penal Code, highlighting the form's dual purpose as both a medical and legal document within the framework of occupational health in corrections facilities.
| Question | Answer |
|---|---|
| Form Name | Form Cdc 7336 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | cdc 2 step tb skin test form printable, cdcr7336 form, cdc7336, cdcr form 7336 |
