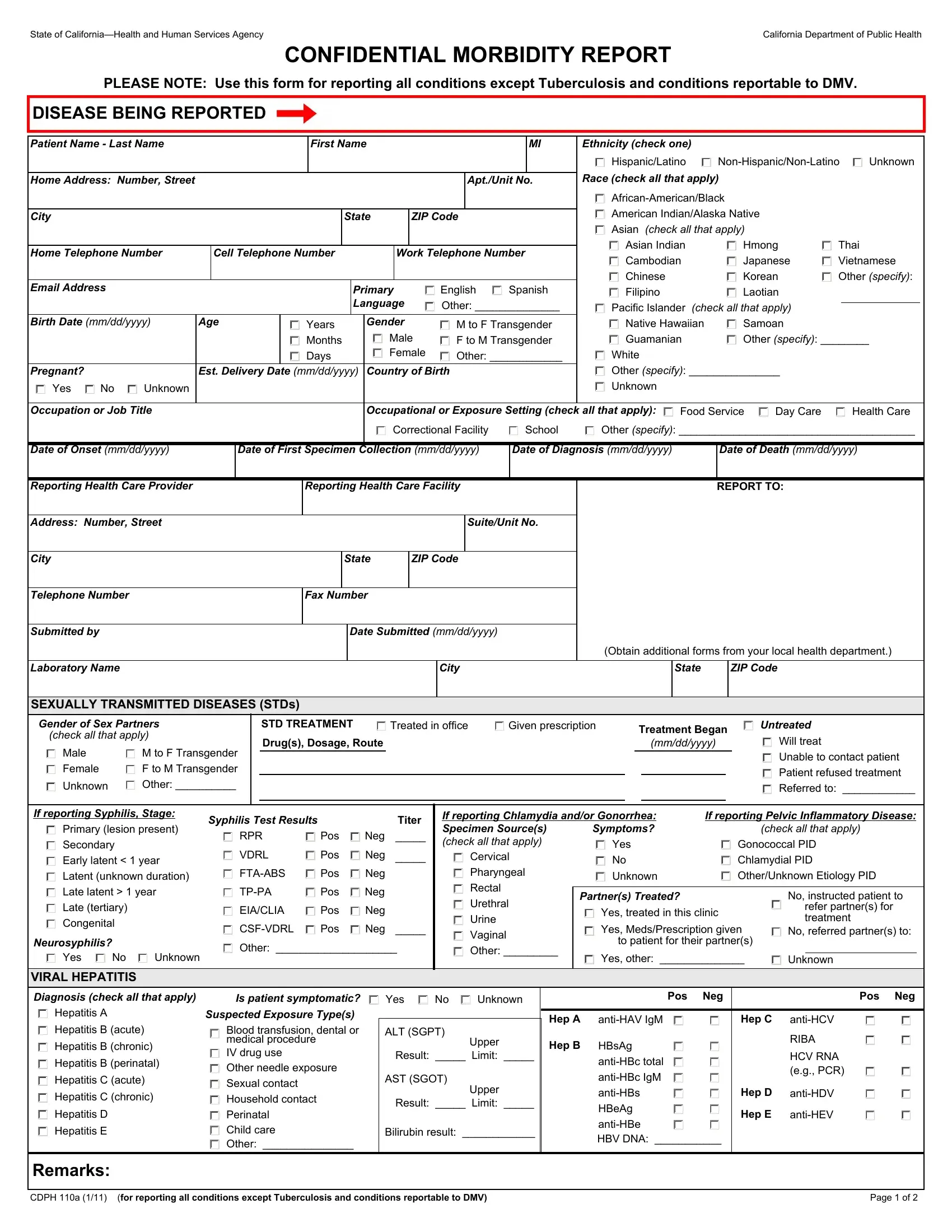
In the complex landscape of public health reporting and management, the CDPH 110A form emerges as a critical document within California's healthcare infrastructure. Designed and mandated by the State of California—Health and Human Services Agency, and specifically utilized by the California Department of Public Health, this form assumes a vital role in the confidential morbidity reporting process. It stipulates a structured approach for healthcare professionals to report a wide spectrum of conditions, excluding Tuberculosis and conditions reportable to the Department of Motor Vehicles (DMV). The comprehensive nature of the form captures detailed patient information including but not limited to ethnicity, race, gender, birth details, contact information, and linguistic preference. Significantly, the form delves into specifics regarding the disease being reported, exposure settings, onset and diagnosis dates, and detailed treatment information for sexually transmitted diseases (STDs), as well as viral hepatitis—highlighting its pivotal role in disease surveillance and public health initiative. Equally important is the section dedicated to the reporting healthcare provider and facility, ensuring a clear channel for communication and follow-up. This intricate form not only facilitates a systematic reporting to health authorities but also underscores the importance of accurate data collection in implementing effective public health strategies and interventions.
| Question | Answer |
|---|---|
| Form Name | Form Cdph 110A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CMRcdph0110a confidential morbidity report san bernardino county form |
