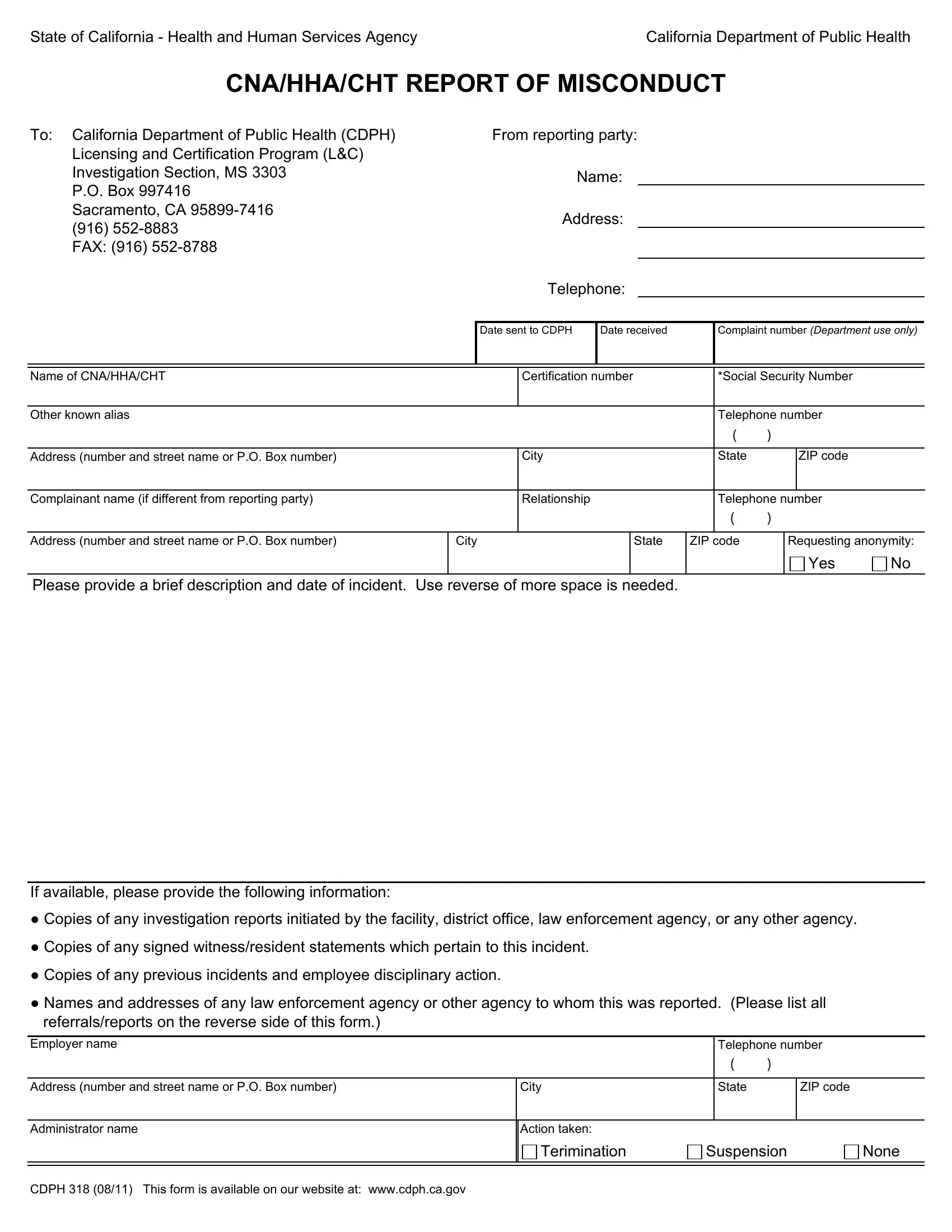
In a world where the integrity of healthcare services is paramount, the State of California - Health and Human Services Agency California Department of Public Health has instituted a robust mechanism to oversee the conduct of Certified Nursing Assistants (CNAs), Home Health Aides (HHAs), and Certified Hemodialysis Technicians (CHTs) through the CNA/HHA/CHT Report of Misconduct form, CDPH 318. Designed to streamline the reporting of professional misconduct, this document serves a critical role in ensuring that healthcare providers adhere to the highest standards of care and ethics. The form facilitates the structured submission of complaints directly to the CDPH's Licensing and Certification Program Investigation Section, providing a thorough channel for the reporting party to outline the incident, include relevant documentation such as investigation reports, witness statements, and information about any prior incidents. Additionally, it captures details about the actions taken by the employer and reports made to other regulatory or law enforcement agencies, reinforcing the collaborative effort between the CDPH and other bodies in maintaining the integrity of health services in California. Importantly, the form also addresses the privacy of the individuals involved by making provisions for anonymity and detailing the use of sensitive information such as social security numbers, thereby balancing accountability with respect for privacy. Overall, the CDPH 318 form is a testament to California's commitment to high-quality healthcare delivery and the protection of its beneficiaries.
| Question | Answer |
|---|---|
| Form Name | Form Cdph 318 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | cdph318 cnahhacht form |
State of California - Health and Human Services Agency |
California Department of Public Health |
CNA/HHA/CHT REPORT OF MISCONDUCT
To: California Department of Public Health (CDPH)
Licensing and Certification Program (L&C)
Investigation Section, MS 3303
P.O. Box 997416
Sacramento, CA
(916)
FAX: (916)
From reporting party:
Name:
Address:
Telephone:
Date sent to CDPH |
Date received |
Complaint number (Department use only) |
|
|
|
Name of CNA/HHA/CHT |
|
Certification number |
|
|
*Social Security Number |
|
||||
|
|
|
|
|
|
|
|
|
|
|
Other known alias |
|
|
|
|
|
Telephone number |
|
|||
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address (number and street name or P.O. Box number) |
|
City |
|
|
State |
|
|
ZIP code |
|
|
|
|
|
|
|
|
|
|
|
|
|
Complainant name (if different from reporting party) |
|
Relationship |
|
|
Telephone number |
|
||||
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address (number and street name or P.O. Box number) |
City |
|
State |
ZIP code |
|
Requesting anonymity: |
||||
|
|
|
|
|
|
|
|
|
Yes |
No |
Please provide a brief description and date of incident. Use reverse of more space is needed.
If available, please provide the following information:
●Copies of any investigation reports initiated by the facility, district office, law enforcement agency, or any other agency.
●Copies of any signed witness/resident statements which pertain to this incident.
●Copies of any previous incidents and employee disciplinary action.
●Names and addresses of any law enforcement agency or other agency to whom this was reported. (Please list all referrals/reports on the reverse side of this form.)
Employer name |
|
|
Telephone number |
||
|
|
|
( |
) |
|
|
|
|
|
|
|
Address (number and street name or P.O. Box number) |
City |
|
State |
|
ZIP code |
|
|
|
|
|
|
Administrator name |
Action taken: |
|
|
|
|
|
Terimination |
Suspension |
None |
||
|
|
|
|
|
|
|
|
|
|
|
|
CDPH 318 (08/11) This form is available on our website at: www.cdph.ca.gov
Reported to:
LICENSING AND CERTIFICATION DISTRICT OFFICE |
|
Date |
|
|
|
|
|
|
|
Address (number and street name or P.O. Box number) |
City |
State |
|
ZIP code |
|
|
|
|
|
Name of individual reported to |
|
Telephone number |
||
|
|
( |
) |
|
|
|
|
|
|
Complaint investigation conducted?
Yes
No |
If yes, date: |
LAW ENFORCEMENT AGENCY |
|
Date |
|
|
|
|
|
|
|
Address (number and street name or P.O. Box number) |
City |
State |
|
ZIP code |
|
|
|
|
|
Name of individual reported to |
|
Telephone number |
||
|
|
( |
) |
|
|
|
|
|
|
Complaint investigation conducted?
Yes
No |
If yes, date: |
Did it result in an arrest:
Yes |
No |
Report number
OMBUDSMAN |
|
Date |
|
|
|
|
|
|
|
Address (number and street name or P.O. Box number) |
City |
State |
|
ZIP code |
|
|
|
|
|
Name of individual reported to |
|
Telephone number |
||
|
|
( |
) |
|
|
|
|
|
|
Complaint investigation conducted?
Yes
No |
If yes, date: |
BUREAU OF |
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
Address (number and street name or P.O. Box number) |
|
|
City |
State |
|
ZIP code |
||
|
|
|
|
|
|
|
|
|
Name of individual reported to |
|
|
|
|
|
Telephone number |
||
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
Complaint investigation conducted? |
|
|
|
|
|
|
|
|
Yes |
No |
If yes, date: |
|
|
|
|||
|
|
|
|
|
|
|
|
|
Complaint description (continued).
INFORMATION COLLECTION AND ACCESS: PRIVACY STATEMENT
*Social Security Number Disclosure: Pursuant to Section 666(a)(13) of Title 42 of the United States Code and California Family Code, Section 17520, subdivision (d), the California Department of Public Health (CDPH), is required to collect social security numbers from all applicants for nursing assistant certificates, home health aide certificates, hemodialysis technician certificates or nursing home administrator licenses. Disclosure of your social security number is mandatory for purposes of establishing, modifying, or enforcing child support orders upon request by the Health Integrity and Protection Data Bank as required by 45 CFR §61.1 et seq . Failure to provide your social security number will result in the return of your application. Your social security number will be used by CDPH for internal identification, and may be used to verify information on your application, to verify certification with another state's certification authority, for examination identification, for identification purposes in national disciplinary databases or as the basis of a disciplinary action against you.
Note: Reports made to the Investigation Section will be coordinated with other agencies.
CDPH 318 (08/11) This form is available on our website at: www.cdph.ca.gov