

Form Cdph 4453 can be completed online easily. Just use FormsPal PDF editing tool to finish the job quickly. To have our tool on the leading edge of practicality, we work to implement user-driven capabilities and improvements regularly. We are always glad to get suggestions - join us in revolutionizing the way you work with PDF files. To get the ball rolling, take these basic steps:
Step 1: Press the orange "Get Form" button above. It is going to open our editor so that you can start completing your form.
Step 2: This editor helps you modify your PDF in many different ways. Change it by writing any text, correct what is originally in the document, and include a signature - all within a few clicks!
Completing this form needs attention to detail. Make sure every field is filled out correctly.
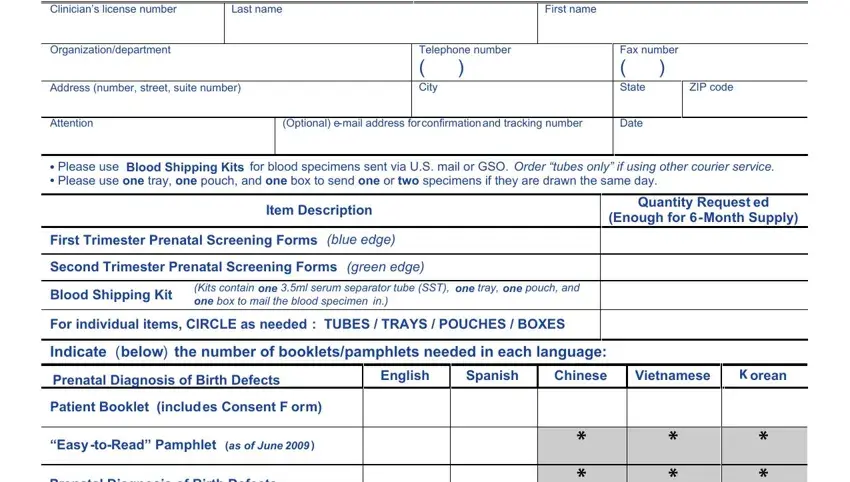
1. Complete the Form Cdph 4453 with a number of major blank fields. Collect all of the necessary information and make sure absolutely nothing is missed!
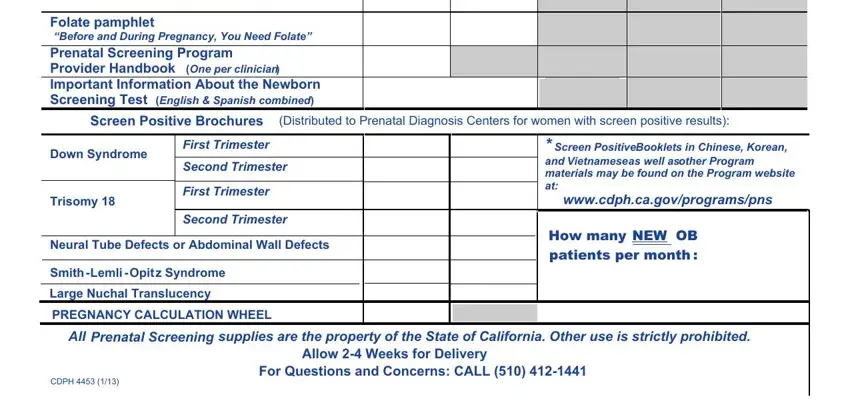
2. The third part is to submit the following fields: Folate pamphlet Before and During, Screen Positive Brochures, Distributed to Prenatal Diagnosis, Down Syndrome, Trisomy, First Trimester, Second Trimester, First Trimester, Second Trimester, Neural Tube Defects or Abdominal, Smith Lemli Opit z Syndrome, Large Nuchal Translucency, PREGNANCY CALCULATION WHEEL, Screen Positive Booklets in, and wwwcdphcagovprogramspns.
3. This next portion is mostly about California Department of Public, Name of laboratorydraw station, Organizationdepartment, Address number street suite number, Telephone number City, Fax number State, ZIP code, Attention, Optional email address for, Date, Please use Blood Shipping Kits, Item Description, Quantity Request ed, Enough for Month Supply, and Blood Shipping Kit - fill in all these blank fields.
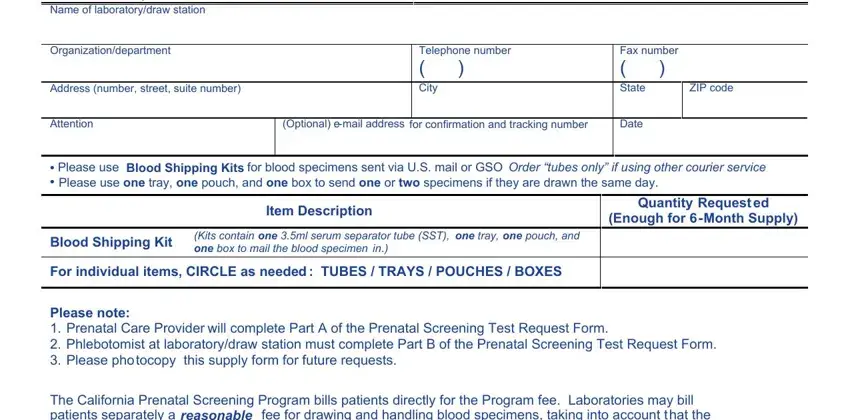
Always be very attentive while filling out Fax number State and Name of laboratorydraw station, since this is where a lot of people make mistakes.
Step 3: Proofread everything you have typed into the blanks and then click on the "Done" button. Create a free trial account with us and obtain direct access to Form Cdph 4453 - readily available from your FormsPal account. FormsPal guarantees your data privacy by having a protected method that never records or shares any type of sensitive information typed in. Be assured knowing your paperwork are kept safe each time you work with our editor!