
You are able to complete Form Cdph 502 effectively by using our online editor for PDFs. Our editor is constantly evolving to grant the very best user experience attainable, and that's because of our resolve for continual enhancement and listening closely to customer comments. Here's what you would need to do to get started:
Step 1: Open the PDF file in our tool by clicking on the "Get Form Button" at the top of this webpage.
Step 2: As you launch the file editor, you'll see the form made ready to be filled out. In addition to filling in different blank fields, you may also perform many other actions with the file, that is putting on your own words, editing the initial text, inserting images, affixing your signature to the form, and more.
This PDF form will need particular info to be entered, thus make sure to take your time to provide precisely what is expected:
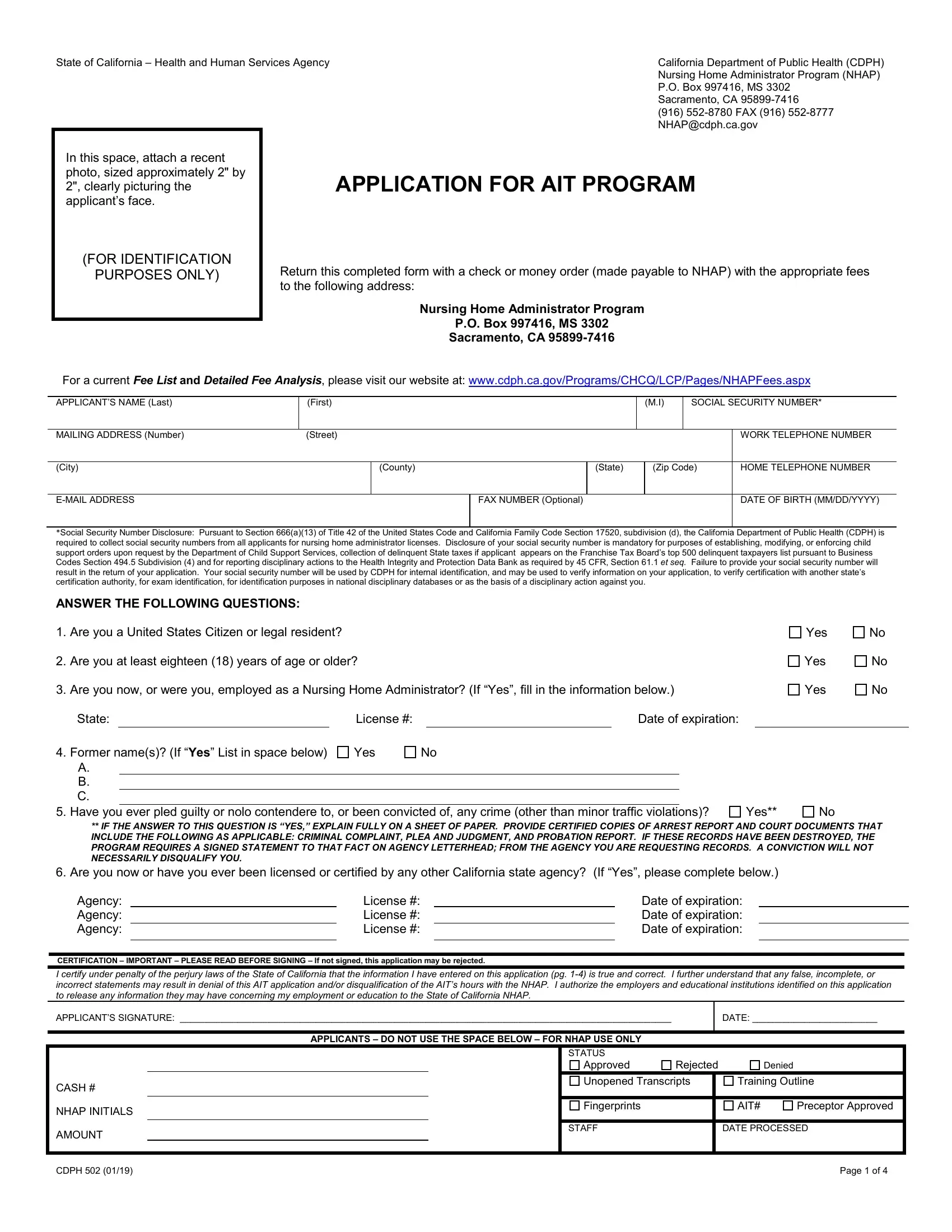
1. The Form Cdph 502 usually requires particular details to be entered. Be sure that the next fields are filled out:
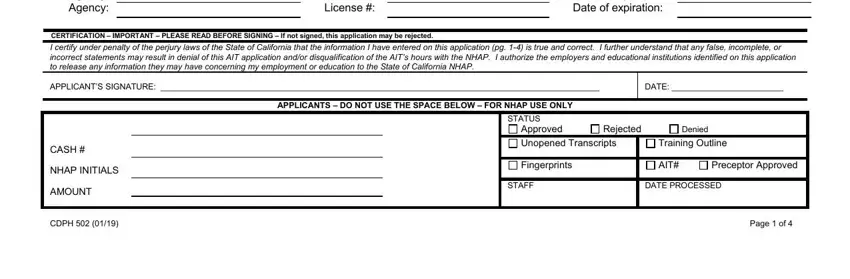
2. Just after performing the last step, go to the next stage and fill in the essential details in these blank fields - Agency Agency Agency, License License License, Date of expiration Date of, CERTIFICATION IMPORTANT PLEASE, I certify under penalty of the, APPLICANTS SIGNATURE, DATE, APPLICANTS DO NOT USE THE SPACE, CASH, NHAP INITIALS, AMOUNT, CDPH, STATUS, Approved, and Rejected.
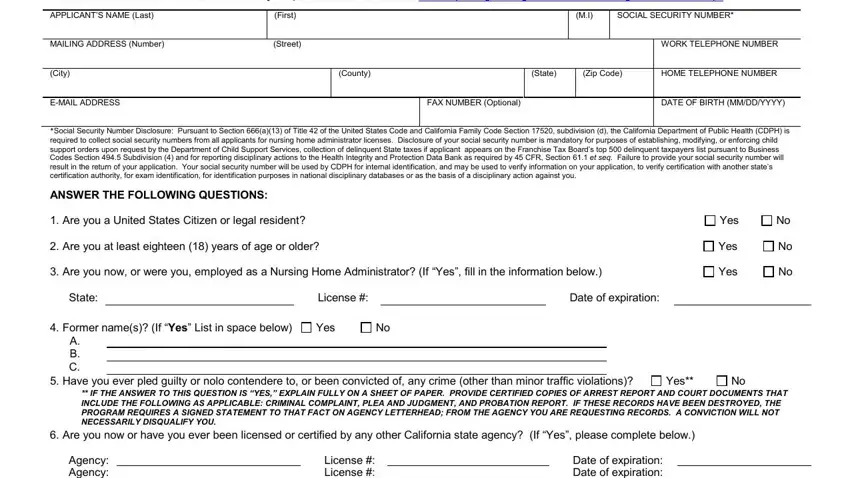
3. This next segment is usually quite easy, APPLICANTS NAME Last, First, SOCIAL SECURITY NUMBER, EDUCATION, DID YOU GRADUATE FROM HIGH SCHOOL, Yes, UNIVERSITY OR COLLEGE NAMEAND, LOCATION BUSINESS CORRESPONDENCE, IF NOT DO YOU POSSESS A GED OR, IF NOT ENTER THE HIGHEST GRADE YOU, Yes, COURSE, UNITS, SEMESTER, and QUARTER - these form fields is required to be filled out here.
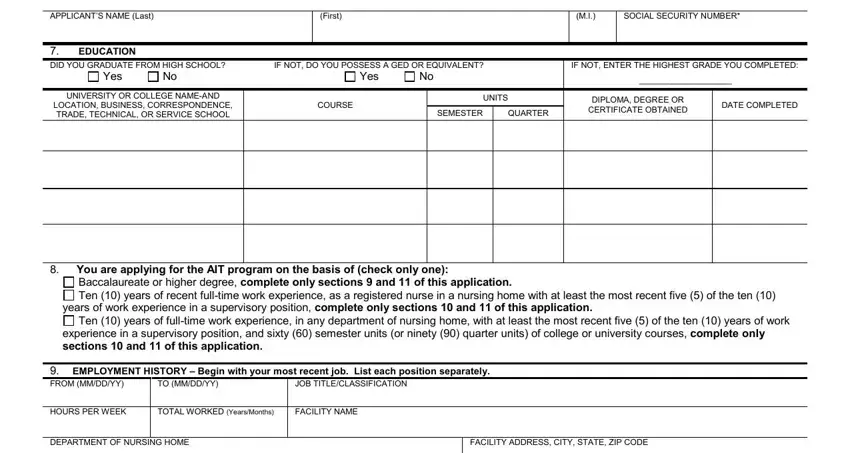
4. The next part will require your input in the subsequent places: DUTIES AND RESPONSIBILITIES, FROM MMDDYY, TO MMDDYY, JOB TITLECLASSIFICATION, HOURS PER WEEK, TOTAL WORKED YearsMonths, FACILITY NAME, DEPARTMENT OF NURSING HOME, FACILITY ADDRESS CITY STATE ZIP, and DUTIES AND RESPONSIBILITIES. Make certain to enter all required details to move forward.
Lots of people frequently make some mistakes when completing FACILITY ADDRESS CITY STATE ZIP in this section. Remember to review whatever you enter here.
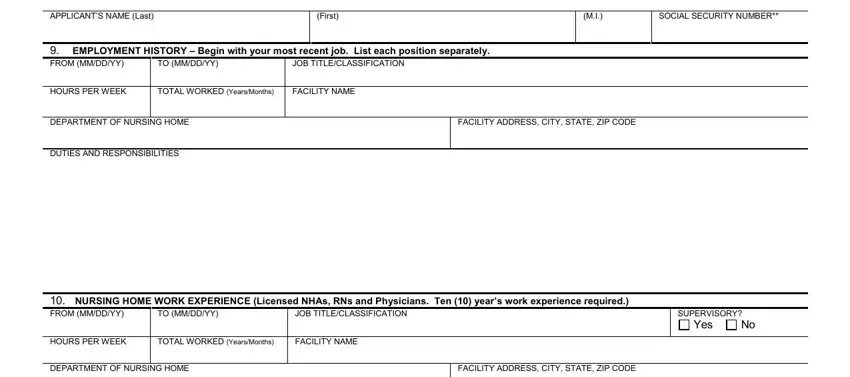
5. To finish your document, the final segment has some additional blanks. Typing in APPLICANTS NAME Last, First, SOCIAL SECURITY NUMBER, FROM MMDDYY, EMPLOYMENT HISTORY Begin with, TO MMDDYY, JOB TITLECLASSIFICATION, HOURS PER WEEK, TOTAL WORKED YearsMonths, FACILITY NAME, DEPARTMENT OF NURSING HOME, FACILITY ADDRESS CITY STATE ZIP, DUTIES AND RESPONSIBILITIES, NURSING HOME WORK EXPERIENCE, and JOB TITLECLASSIFICATION should finalize the process and you'll certainly be done in the blink of an eye!
Step 3: As soon as you've glanced through the details in the blanks, simply click "Done" to finalize your document creation. After creating afree trial account here, you will be able to download Form Cdph 502 or send it via email promptly. The PDF file will also be available from your personal cabinet with your edits. FormsPal offers risk-free document completion devoid of personal information recording or any sort of sharing. Rest assured that your information is safe with us!