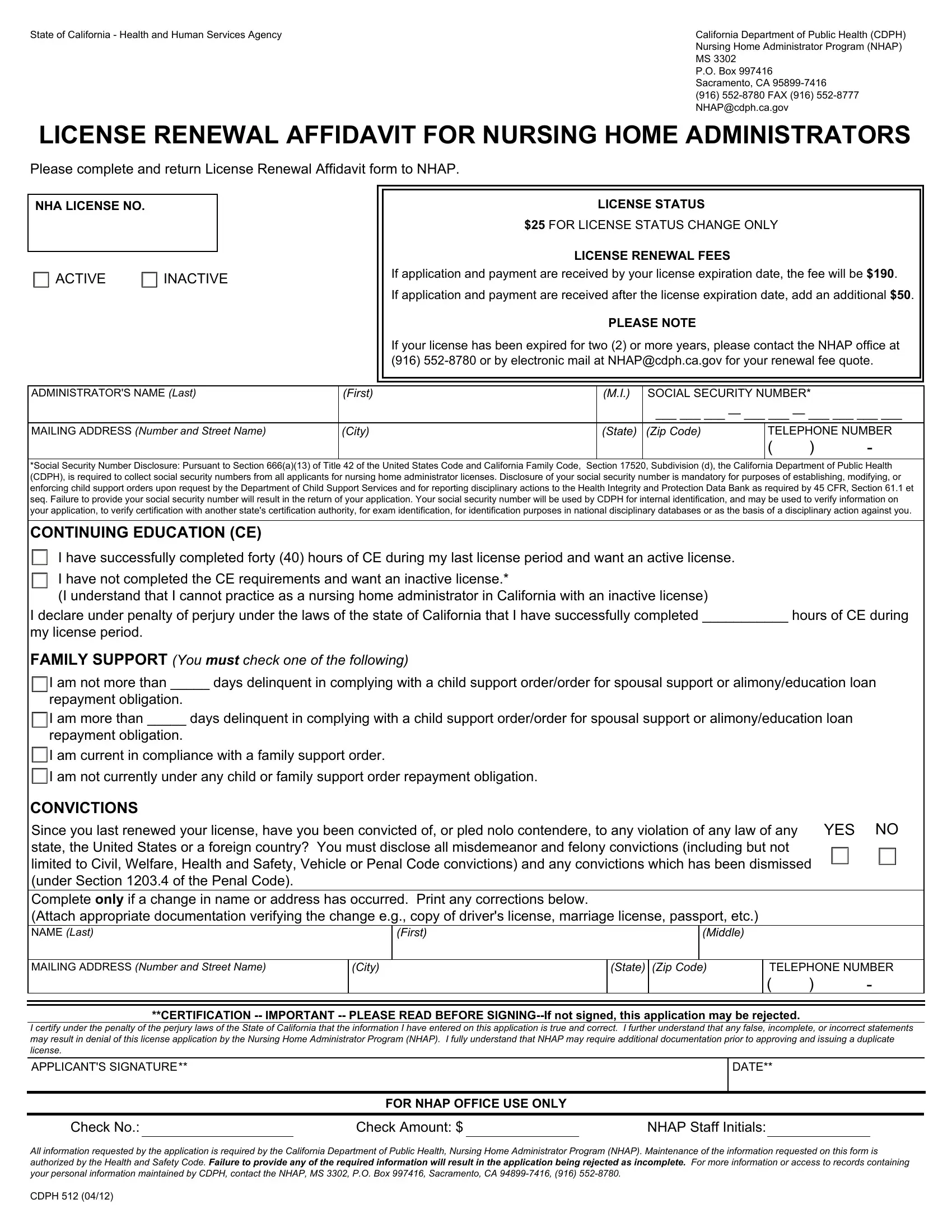
The CDPH 512 form is a critical document for nursing home administrators in California, playing a pivotal role in the maintenance and renewal of their professional licenses. Managed by the California Department of Public Health's Nursing Home Administrator Program (NHAP), this form serves as a comprehensive affidavit for license renewal, outlining a series of requirements and actions needed from the administrators. One of the key aspects of the form is its section on license renewal fees, which details the costs involved if applications and payments are submitted by or after the expiration date of the existing license. Importantly, the form also requires disclosure of the administrator’s social security number, underpinned by federal and state regulations to support child support enforcement and to comply with disciplinary reporting obligations. Moreover, it emphasizes the necessity for administrators to have completed a stipulated amount of Continuing Education (CE) hours, differentiating between those seeking active versus inactive license status. Inclusion of a section for family support compliance indicates the state's effort to ensure professionals are meeting their personal legal responsibilities. Furthermore, the form inquires about any convictions that may have occurred since the last renewal, underscoring the integrity and accountability expected of nursing home administrators. Finally, any changes in the administrator’s personal details, such as name or address, must be accurately reflected and accompanied by the appropriate verification documentation. This form, demanding honesty and thoroughness, ultimately represents a key step in ensuring that only qualified individuals are at the helm of nursing home administration in California.
| Question | Answer |
|---|---|
| Form Name | Form Cdph 512 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cdph512 affadavit form for change to nursing home license |
State of California - Health and Human Services Agency |
California Department of Public Health (CDPH) |
|
Nursing Home Administrator Program (NHAP) |
|
MS 3302 |
|
P.O. Box 997416 |
|
Sacramento, CA |
|
(916) |
|
NHAP@cdph.ca.gov |
LICENSE RENEWAL AFFIDAVIT FOR NURSING HOME ADMINISTRATORS
Please complete and return License Renewal Affidavit form to NHAP.
NHA LICENSE NO.
ACTIVE INACTIVE
LICENSE STATUS
$25 FOR LICENSE STATUS CHANGE ONLY
LICENSE RENEWAL FEES
If application and payment are received by your license expiration date, the fee will be $190.
If application and payment are received after the license expiration date, add an additional $50.
PLEASE NOTE
If your license has been expired for two (2) or more years, please contact the NHAP office at (916)
ADMINISTRATOR'S NAME (Last) |
(First) |
(M.I.) |
SOCIAL SECURITY NUMBER* |
|
||
|
|
|
___ ___ ___ — ___ ___ — ___ ___ ___ ___ |
|||
|
|
|
|
|
||
MAILING ADDRESS (Number and Street Name) |
(City) |
(State) |
(Zip Code) |
TELEPHONE NUMBER |
||
|
|
|
|
( |
) |
- |
|
|
|
|
|
|
|
*Social Security Number Disclosure: Pursuant to Section 666(a)(13) of Title 42 of the United States Code and California Family Code, Section 17520, Subdivision (d), the California Department of Public Health (CDPH), is required to collect social security numbers from all applicants for nursing home administrator licenses. Disclosure of your social security number is mandatory for purposes of establishing, modifying, or enforcing child support orders upon request by the Department of Child Support Services and for reporting disciplinary actions to the Health Integrity and Protection Data Bank as required by 45 CFR, Section 61.1 et seq. Failure to provide your social security number will result in the return of your application. Your social security number will be used by CDPH for internal identification, and may be used to verify information on your application, to verify certification with another state's certification authority, for exam identification, for identification purposes in national disciplinary databases or as the basis of a disciplinary action against you.
CONTINUING EDUCATION (CE)
I have successfully completed forty (40) hours of CE during my last license period and want an active license.
I have not completed the CE requirements and want an inactive license.*
(I understand that I cannot practice as a nursing home administrator in California with an inactive license)
I declare under penalty of perjury under the laws of the state of California that I have successfully completed ___________ hours of CE during
my license period.
FAMILY SUPPORT (You must check one of the following)
I am not more than _____ days delinquent in complying with a child support order/order for spousal support or alimony/education loan
repayment obligation.
I am more than _____ days delinquent in complying with a child support order/order for spousal support or alimony/education loan
repayment obligation.
I am current in compliance with a family support order.
I am not currently under any child or family support order repayment obligation.
CONVICTIONS
Since you last renewed your license, have you been convicted of, or pled nolo contendere, to any violation of any law of any |
YES NO |
state, the United States or a foreign country? You must disclose all misdemeanor and felony convictions (including but not |
|
limited to Civil, Welfare, Health and Safety, Vehicle or Penal Code convictions) and any convictions which has been dismissed |
|
(under Section 1203.4 of the Penal Code). |
|
|
|
Complete only if a change in name or address has occurred. Print any corrections below. |
|
(Attach appropriate documentation verifying the change e.g., copy of driver's license, marriage license, passport, etc.) |
|
NAME (Last)
(First)
(Middle)
MAILING ADDRESS (Number and Street Name)
(City)
(State) (Zip Code)
TELEPHONE NUMBER
( |
) |
- |
**CERTIFICATION
I certify under the penalty of the perjury laws of the State of California that the information I have entered on this application is true and correct. I further understand that any false, incomplete, or incorrect statements may result in denial of this license application by the Nursing Home Administrator Program (NHAP). I fully understand that NHAP may require additional documentation prior to approving and issuing a duplicate license.
APPLICANT'S SIGNATURE**
DATE**
FOR NHAP OFFICE USE ONLY
Check No.: |
|
Check Amount: $ |
|
NHAP Staff Initials: |
All information requested by the application is required by the California Department of Public Health, Nursing Home Administrator Program (NHAP). Maintenance of the information requested on this form is authorized by the Health and Safety Code. Failure to provide any of the required information will result in the application being rejected as incomplete. For more information or access to records containing your personal information maintained by CDPH, contact the NHAP, MS 3302, P.O. Box 997416, Sacramento, CA
CDPH 512 (04/12)