Navigating the intricacies of the CDPH 516 form is crucial for those stepping into the role of a nursing home administrator or further consolidating their credentials within the state of California. This form, an integral part of the California Department of Public Health's Nursing Home Administrator Program (NHAP), serves as a registration form for preceptor training—a mandatory step for nursing home administrators aiming to either attain or maintain their license and enhance their professional development. The form is not just a mere document; it encapsulates the aspirant's commitment to upholding the highest standards of care and administrative acumen in nursing homes. With sections ranging from personal information, qualifications that earmark an individual's eligibility to be a preceptor, to the specifics about training sessions and legal attestations regarding past convictions, it is both comprehensive and sensitive in nature. Moreover, the inclusion of associated fees, requirements for continued education credit, and renewal terms underlines the form's pivotal role in ensuring that administrators are not only qualified but also continuously aligned with evolving best practices in the sphere of nursing home administration. The requirement to disclose a social security number, driven by legal mandates aimed at enforcing child support orders and reporting disciplinary actions, underscores the form's role in fostering transparency and accountability within the healthcare system. Understanding the multifaceted aspects and the underlying importance of the CDPH 516 form offers a window into the rigorous standards and preparatory pathways that define the realm of nursing home administration in California.
| Question | Answer |
|---|---|
| Form Name | Form Cdph 516 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | false, California, cdph nursing home administrator program, nursing home administrator preceptor california |
State of California - Health and Human Services Agency |
California Department of Public Health (CDPH) |
|
Nursing Home Administrator Program (NHAP) |
|
MS 3302 |
|
P.O. Box 997416 |
|
Sacramento, CA |
|
(916) |
|
NHAP@cdph.ca.gov |
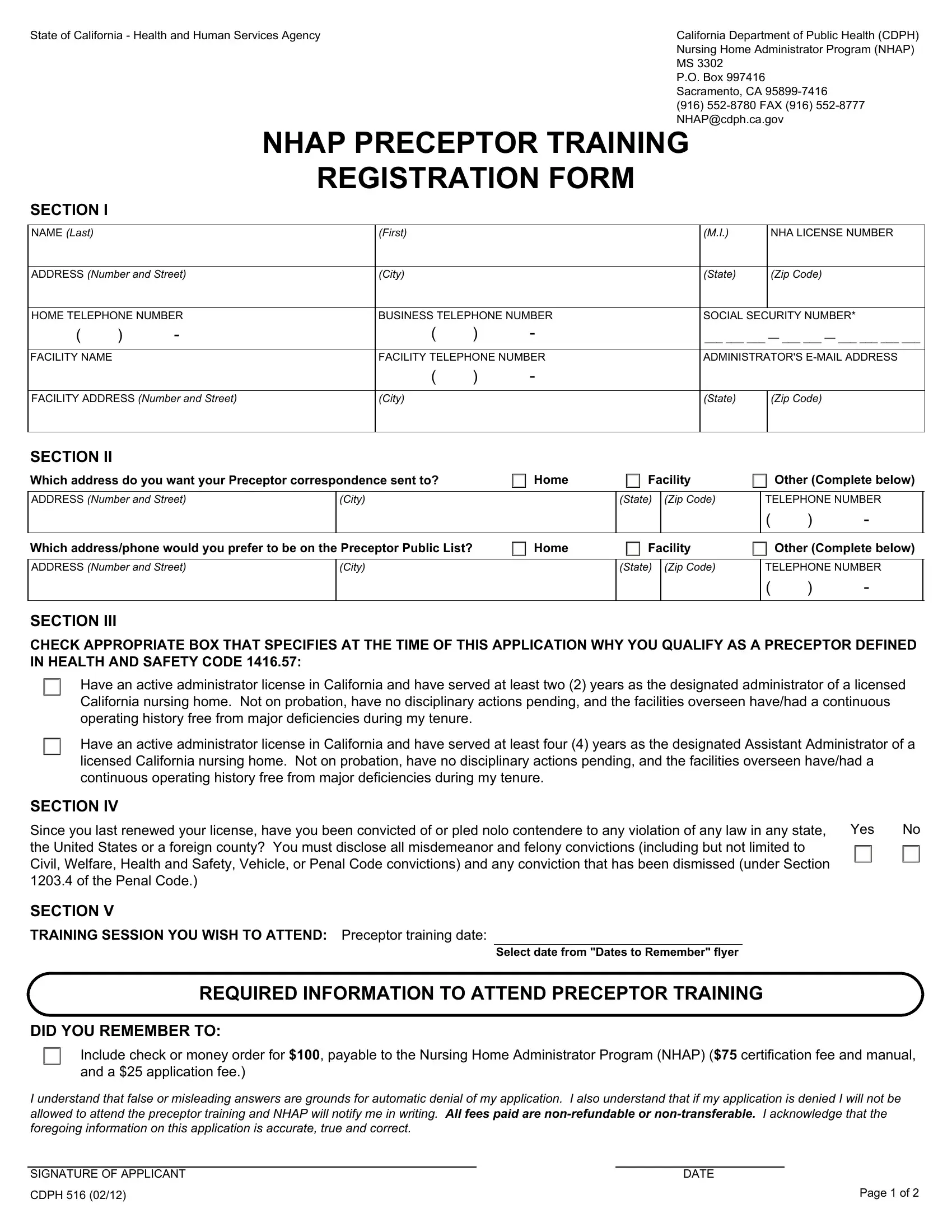
NHAP PRECEPTOR TRAINING
REGISTRATION FORM
SECTION I
NAME (Last) |
|
|
(First) |
|
|
|
(M.I.) |
NHA LICENSE NUMBER |
|
|
|
|
|
|
|
||
ADDRESS (Number and Street) |
(City) |
|
|
|
(State) |
(Zip Code) |
||
|
|
|
|
|
||||
HOME TELEPHONE NUMBER |
BUSINESS TELEPHONE NUMBER |
|
SOCIAL SECURITY NUMBER* |
|||||
( |
) |
- |
( |
) |
- |
|
___ ___ ___ — ___ ___ — ___ ___ ___ ___ |
|
|
|
|
|
|
|
|
||
FACILITY NAME |
|
|
FACILITY TELEPHONE NUMBER |
|
ADMINISTRATOR'S |
|||
|
|
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
|
||
FACILITY ADDRESS (Number and Street) |
(City) |
|
|
|
(State) |
(Zip Code) |
||
|
|
|
|
|
|
|
|
|
SECTION II |
|
|
|
|
|
|
|
|
Which address do you want your Preceptor correspondence sent to? |
|
Home |
Facility |
Other (Complete below) |
||||
ADDRESS (Number and Street)
(City)
(State) (Zip Code)
TELEPHONE NUMBER
( |
) |
- |
Which address/phone would you prefer to be on the Preceptor Public List? |
Home |
Facility |
Other (Complete below) |
ADDRESS (Number and Street)
(City)
(State) (Zip Code)
TELEPHONE NUMBER
( |
) |
- |
SECTION III
CHECK APPROPRIATE BOX THAT SPECIFIES AT THE TIME OF THIS APPLICATION WHY YOU QUALIFY AS A PRECEPTOR DEFINED IN HEALTH AND SAFETY CODE 1416.57:
Have an active administrator license in California and have served at least two (2) years as the designated administrator of a licensed California nursing home. Not on probation, have no disciplinary actions pending, and the facilities overseen have/had a continuous operating history free from major deficiencies during my tenure.
Have an active administrator license in California and have served at least four (4) years as the designated Assistant Administrator of a licensed California nursing home. Not on probation, have no disciplinary actions pending, and the facilities overseen have/had a continuous operating history free from major deficiencies during my tenure.
SECTION IV
Since you last renewed your license, have you been convicted of or pled nolo contendere to any violation of any law in any state, |
Yes |
No |
the United States or a foreign county? You must disclose all misdemeanor and felony convictions (including but not limited to |
|
|
Civil, Welfare, Health and Safety, Vehicle, or Penal Code convictions) and any conviction that has been dismissed (under Section |
|
|
1203.4 of the Penal Code.) |
|
|
SECTION V
TRAINING SESSION YOU WISH TO ATTEND: Preceptor training date:
Select date from "Dates to Remember" flyer
REQUIRED INFORMATION TO ATTEND PRECEPTOR TRAINING
DID YOU REMEMBER TO:
Include check or money order for $100, payable to the Nursing Home Administrator Program (NHAP) ($75 certification fee and manual, and a $25 application fee.)
I understand that false or misleading answers are grounds for automatic denial of my application. I also understand that if my application is denied I will not be allowed to attend the preceptor training and NHAP will notify me in writing. All fees paid are
SIGNATURE OF APPLICANT |
|
DATE |
|
CDPH 516 (02/12) |
|
|
Page 1 of 2 |
SECTION I Complete this section. All information requested is required.
SECTION II Complete this section. Indicate the specific address information.
SECTION III Check the appropriate box that qualifies you to participate in the training.
SECTION IV |
Check the appropriate box indicating response for conviction statement and NHA Profile Sheet. |
SECTION V Check the box indicating which training session you plan to attend. Sign and date the form.
.
.
.
IMPORTANT INFORMATION
Registration and fee must be postmarked by final filling dates for processing (see Section V). Applications received after the postmarked date will be denied. Fees submitted are
Six (6) hours of continuing education credit will be granted for attending the Preceptor Training.
Preceptor certificates must be renewed every three (3) years from issuance date.
REQUIRED INFORMATION
*Social Security Number Disclosure: Pursuant to Section 666(a)(13) of Title 42 of the United States Code and California Family Code, Section 17520, Subdivision (d), the California Department of Public Health (CDPH), is required to collect social security numbers from all applicants for nursing home administrator licenses. Disclosure of your social security number is mandatory for purposes of establishing, modifying, or enforcing child support orders upon request by the Department of Child Support Services and for reporting disciplinary actions to the Health Integrity and Protection Data Bank as required by 45 CFR, Section 61.1 et seq.
Failure to provide your social security number will result in the return of your application. Your social security number will be used by CDPH for internal identification, and may be used to verify information on your application, to verify certification with another state's certification authority, for exam identification, for identification purposes in national disciplinary databases or as the basis of a disciplinary action against you.
STATUTES THAT GOVEN THE NURSING HOME ADMINISTRATOR PROGRAM
Health and Safety Code, Section 1416, Nursing Home Administrator Program.
FOR OFFICE USE ONLY
Check/M.O. #: |
|
|
Amount $: |
|
|
|
NHAP STAFF INITIALS: |
|
|
||||
Issue Date: |
|
|
Expiration Date: |
|
|
Session Date: |
|
|
|||||
CF#: |
|
|
PRE#: |
|
|
|
CE#: |
|
|||||
CDPH 516 (02/12) |
Page 2 of 2 |