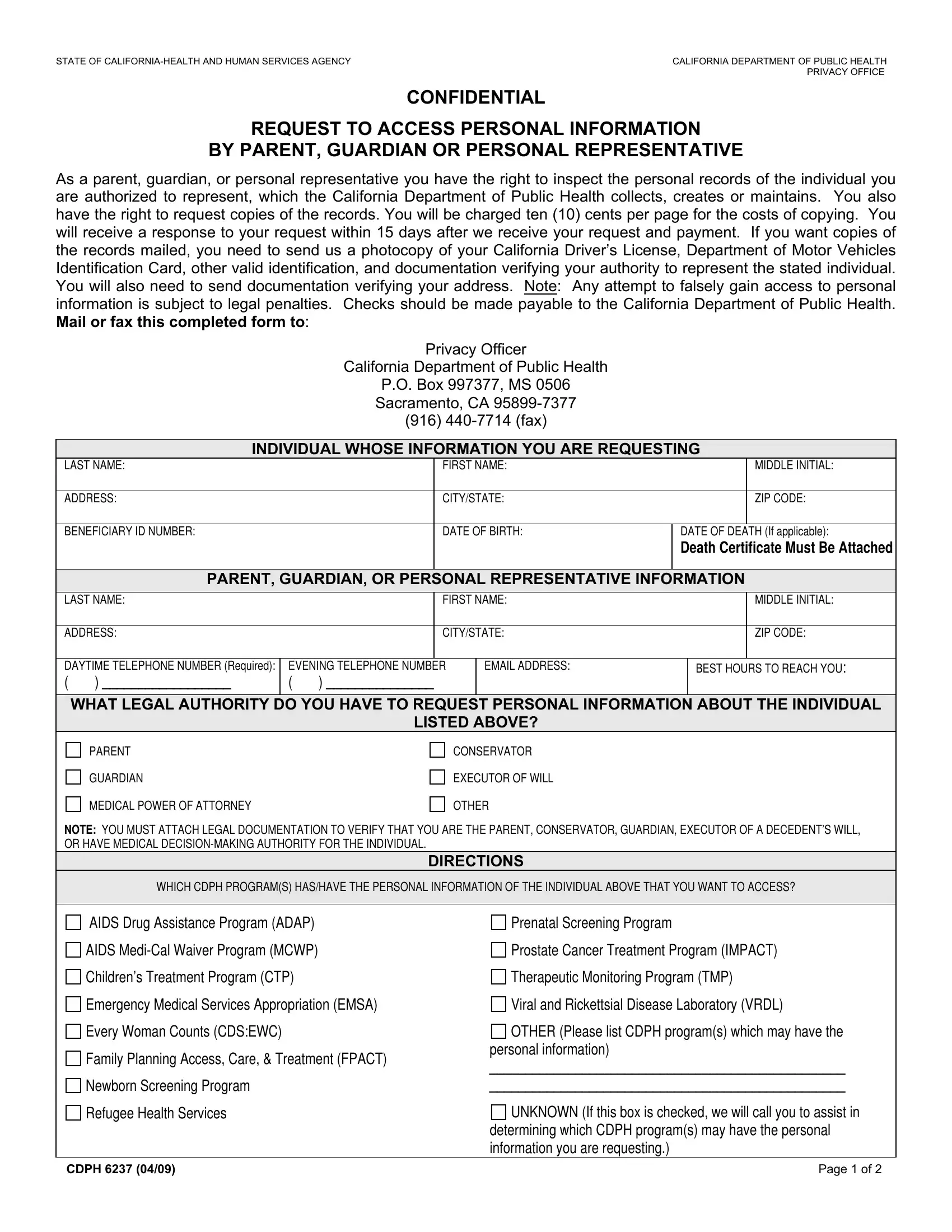
In today’s age of heightened awareness around privacy and the secure handling of personal information, the State of California Health and Human Services Agency, through the California Department of Public Health (CDPH), provides a structured means for individuals to maintain control over their personal or represented individuals' health records. The CDPH 6237 form plays a pivotal role in this process. Designed as a formal request to access personal information, it is specifically geared towards parents, guardians, or personal representatives who have a legal right to inspect or obtain copies of health records managed by the CDPH. The completion and submission of this form initiate a clear channel to not only examine these records but also to receive copies, with a charge applied per page for such copies. Within a stipulated timeframe, typically 15 days upon receipt and processing of the request along with the corresponding payment, the applicant is promised a response. The form meticulously requires the submission of identification and authorization verification to prevent unauthorized access, underscoring the CDPH’s commitment to safeguarding personal health information against misuse. Furthermore, it outlines the fees, addresses for mailing or faxing the completed form, and specifies the legal documentation needed to support the request—acting as a comprehensive guide for those navigating the intersection of legal guardianship and health information privacy.
| Question | Answer |
|---|---|
| Form Name | Form Cdph 6237 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CDPH_6237_Acces s_Rep_4 09 printable accesspi checklist form |
STATE OF |
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH |
|
PRIVACY OFFICE |
CONFIDENTIAL
REQUEST TO ACCESS PERSONAL INFORMATION
BY PARENT, GUARDIAN OR PERSONAL REPRESENTATIVE
As a parent, guardian, or personal representative you have the right to inspect the personal records of the individual you are authorized to represent, which the California Department of Public Health collects, creates or maintains. You also have the right to request copies of the records. You will be charged ten (10) cents per page for the costs of copying. You will receive a response to your request within 15 days after we receive your request and payment. If you want copies of the records mailed, you need to send us a photocopy of your California Driver’s License, Department of Motor Vehicles Identification Card, other valid identification, and documentation verifying your authority to represent the stated individual. You will also need to send documentation verifying your address. Note: Any attempt to falsely gain access to personal information is subject to legal penalties. Checks should be made payable to the California Department of Public Health. Mail or fax this completed form to:
Privacy Officer
California Department of Public Health
P.O. Box 997377, MS 0506
Sacramento, CA
(916)
INDIVIDUAL WHOSE INFORMATION YOU ARE REQUESTING
LAST NAME: |
|
FIRST NAME: |
|
|
MIDDLE INITIAL: |
|
|
|
|
|
|
|
|
ADDRESS: |
|
CITY/STATE: |
|
|
ZIP CODE: |
|
|
|
|
|
|
|
|
BENEFICIARY ID NUMBER: |
|
DATE OF BIRTH: |
DATE OF DEATH (If applicable): |
|||
|
|
|
|
DEATH CERTIFICATE MUST BE ATTACHED |
||
|
|
|
|
|
|
|
PARENT, GUARDIAN, OR PERSONAL REPRESENTATIVE INFORMATION |
||||||
LAST NAME: |
|
FIRST NAME: |
|
|
MIDDLE INITIAL: |
|
|
|
|
|
|
|
|
ADDRESS: |
|
CITY/STATE: |
|
|
ZIP CODE: |
|
|
|
|
|
|
|
|
DAYTIME TELEPHONE NUMBER (Required): |
EVENING TELEPHONE NUMBER |
EMAIL ADDRESS: |
|
BEST HOURS TO REACH YOU: |
||
( ) __________________ |
( ) _______________ |
|
|
|
|
|
|
|
|
|
|
|
|
WHAT LEGAL AUTHORITY DO YOU HAVE TO REQUEST PERSONAL INFORMATION ABOUT THE INDIVIDUAL
LISTED ABOVE?
PARENT
GUARDIAN
MEDICAL POWER OF ATTORNEY
CONSERVATOR
EXECUTOR OF WILL
OTHER
NOTE: YOU MUST ATTACH LEGAL DOCUMENTATION TO VERIFY THAT YOU ARE THE PARENT, CONSERVATOR, GUARDIAN, EXECUTOR OF A DECEDENT’S WILL, OR HAVE MEDICAL
DIRECTIONS
WHICH CDPH PROGRAM(S) HAS/HAVE THE PERSONAL INFORMATION OF THE INDIVIDUAL ABOVE THAT YOU WANT TO ACCESS?
AIDS Drug Assistance Program (ADAP)
AIDS
Emergency Medical Services Appropriation (EMSA) Every Woman Counts (CDS:EWC)
Family Planning Access, Care, & Treatment (FPACT) Newborn Screening Program
Refugee Health Services
Prenatal Screening Program
Prostate Cancer Treatment Program (IMPACT)
Therapeutic Monitoring Program (TMP)
Viral and Rickettsial Disease Laboratory (VRDL)
OTHER (Please list CDPH program(s) which may have the personal information)
__________________________________________________
__________________________________________________
UNKNOWN (If this box is checked, we will call you to assist in determining which CDPH program(s) may have the personal information you are requesting.)
CDPH 6237 (04/09) |
Page 1 of 2 |
STATE OF |
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH |
|
PRIVACY OFFICE |
|
I AM REQUESTING COPIES OF RECORDS FOR THE FOLLOWNG DATES |
|
|
YOU MUST SPECIFY DATES IN ORDER TO GET RECORDS |
|
FROM DATE (month/day/year) |
|
TO DATE (month/day/year) |
|
|
|
PLEASE NOTE: FULFILLING A REQUEST FOR RECORDS DATING BACK 6 YEARS AGO OR LESS IS A
PLEASE MAIL ME A COPY OF THE REQUESTED INFORMATION.
I WISH TO REVIEW THE REQUESTED INFORMATION IN PERSON.
IF YOU REQUEST TO REVIEW RECORDS IN PERSON, YOU WILL BE CONTACTED TO SCHEDULE AN APPOINTMENT. LOCATION AVAILABLE FOR IN PERSON REVIEW: SACRAMENTO ONLY
I REQUEST THAT A PERSON OF MY CHOOSING BE ALLOWED TO INSPECT THE RECORDS.
NOTE: Any person or attorney may be named below. Records will not be sent to photocopy services.
NAME: ___________________________________________
RELATIONSHIP TO YOU: ____________________________
TELEPHONE NUMBER: (____) ________________________
ADDRESS: ________________________________________
IDENTIFYING INFORMATION IS REQUIRED
COPY OF ADDRESS VERIFICATION ATTACHED
TYPE: _____________________________ (UTILITY BILL, PHONE BILL, DRIVER’S LICENSE, ETC.)
COPY OF IDENTIFICATION ATTACHED
TYPE: __________________________ (CA DRIVER’S LICENSE, CA DMV IDENTIFICATION CARD, BIRTH CERTIFICATE, BENEFITS IDENTIFICATION CARD, MANAGED
CARE CARD, STATE OR FEDERAL EMPLOYEE ID CARD) NUMBER: ___________________________
(IF NO IDENTIFICATION IS ATTACHED, YOUR SIGNATURE MUST BE NOTARIZED.) NOTARIZED BY ___________________________________ ON ___________________(DATE)
NOTARY PUBLIC NUMBER ________________________________
UNOFFICIAL UNLESS STAMPED BY NOTARY PUBLIC
I DECLARE UNDER PENALTY OF PERJURY THAT THE INFORMATION ON THIS FORM IS TRUE AND CORRECT.
REQUESTING REPRESENTATIVE SIGNATURE: __________________________________________ |
DATE: ______________ |
DEPARTMENT EMPLOYEE PROCESSING/MAINTAINING THIS ACCESS REQUEST
THIS SECTION TO BE COMPLETED BY DEPARTMENT STAFF
(Name and Title)
(Organization within Department) |
(Telephone Number) |
(Mail Stop Number) |
PRIVACY STATEMENT (CA CIVIL CODE SECTION 1798 .17)
THE INFORMATION COLLECTED ON THIS FORM IS USED TO PROCESS YOUR REQUEST FOR ACCESS TO PERSONAL INFORMATION ABOUT AN INDIVIDUAL YOU LEGALLY REPRESENT THAT IS MAINTAINED BY THE CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (DEPARTMENT). THE INFORMATION WE COLLECT FROM YOU ON THIS FORM WILL BE KEPT CONFIDENTIAL AND ON FILE AT THE DEPARTMENT, AS REQUIRED BY LAW. ALL INFORMATION REQUESTED ON THE FORM IS MANDATORY PURSUANT TO CALIFORNIA CIVIL CODE SECTION 1798.32. NOT SUPPLYING THE INFORMATION REQUESTED WILL RESULT IN THE DENIAL OF YOUR REQUEST. ANY INFORMATION PROVIDED MAY BE DISCLOSED TO THE CALIFORNIA STATE AUDITOR, THE CALIFORNIA OFFICE OF HEALTH INFORMATION INTEGRITY, THE CALIFORNIA OFFICE OF INFORMATION SECURITY AND PRIVACY PROTECTION, THE U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES OR TO OTHER STATE AND FEDERAL AGENCIES AS REQUIRED BY LAW.
YOU HAVE THE RIGHT TO REVIEW THE RECORDS WE KEEP ABOUT YOU DURING NORMAL BUSINESS HOURS. THE CALIFORNIA DEPARTMENT OF PUBLIC HEALTH PRIVACY OFFICER WILL, UPON REQUEST, INFORM YOU REGARDING THE LOCATION OF YOUR RECORDS AND THE CATEGORIES OF ANY PERSONS WHO USE THE INFORMATION IN THOSE RECORDS. FOR MORE INFORMATION, CONTACT THE CALIFORNIA DEPARTMENT OF PUBLIC HEALTH, PRIVACY OFFICE, USING THE FOLLOWING CONTACT INFORMATION: CALIFORNIA DEPARTMENT OF PUBLIC HEALTH, OFFICE OF LEGAL SERVICES, PRIVACY OFFICE, MS 0506, P.O. BOX 997377, SACRAMENTO, CALIFORNIA
CDPH 6237 (04/09) |
Page 2 of 2 |