State of California—Health and Human Services Agency |
California Department of Public Health |
|
Food and Drug Branch |
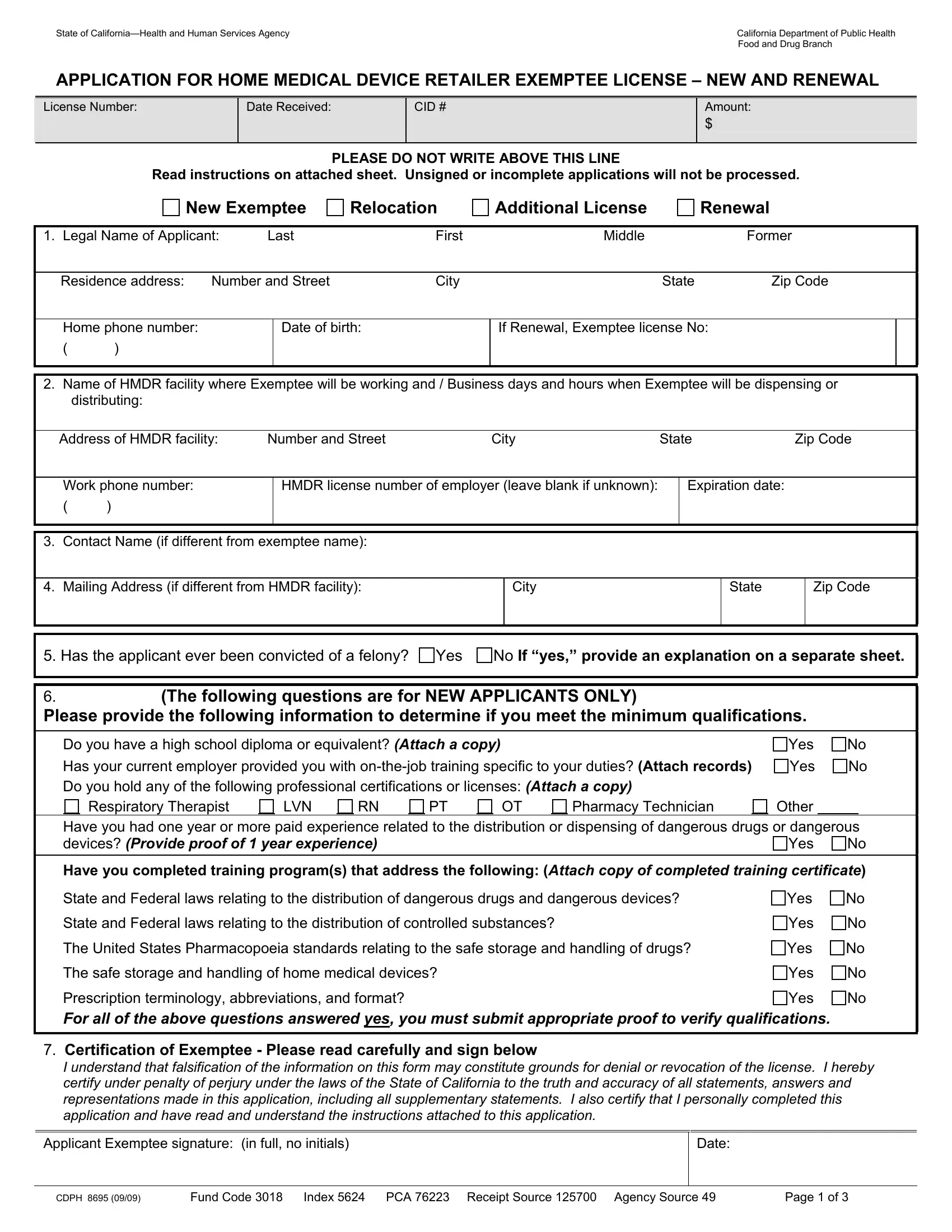
APPLICATION FOR HOME MEDICAL DEVICE RETAILER EXEMPTEE LICENSE – NEW AND RENEWAL
PLEASE DO NOT WRITE ABOVE THIS LINE
Read instructions on attached sheet. Unsigned or incomplete applications will not be processed.
1. |
Legal Name of Applicant: |
Last |
First |
|
Middle |
|
|
Former |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Residence address: |
Number and Street |
City |
|
|
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home phone number: |
|
|
Date of birth: |
|
If Renewal, Exemptee license No: |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
Name of HMDR facility where Exemptee will be working and / Business days and hours when Exemptee will be dispensing or |
|
|
distributing: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address of HMDR facility: |
Number and Street |
|
City |
State |
|
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
Work phone number: |
|
|
HMDR license number of employer (leave blank if unknown): |
|
Expiration date: |
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
Contact Name (if different from exemptee name): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Mailing Address (if different from HMDR facility): |
|
|
City |
|
|
State |
|
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Has the applicant ever been convicted of a felony? Yes |
No If “yes,” provide an explanation on a separate sheet. |
6. |
|
(The following questions are for NEW APPLICANTS ONLY) |
|
|
|
Please provide the following information to determine if you meet the minimum qualifications. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Do you have a high school diploma or equivalent? (Attach a copy) |
|
|
|
|
|
|
Yes |
No |
|
Has your current employer provided you with on-the-job training specific to your duties? (Attach records) |
Yes |
No |
|
Do you hold any of the following professional certifications or licenses: (Attach a copy) |
|
|
|
|
|
Respiratory Therapist |
|
|
LVN |
|
|
RN |
|
|
PT |
|
|
|
OT |
|
|
Pharmacy Technician |
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Have you had one year or more paid experience related to the distribution or dispensing of dangerous drugs or dangerous |
|
devices? (Provide proof of 1 year experience) |
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
Have you completed training program(s) that address the following: (Attach copy of completed training certificate) |
|
State and Federal laws relating to the distribution of dangerous drugs and dangerous devices? |
Yes |
No |
|
State and Federal laws relating to the distribution of controlled substances? |
|
|
|
Yes |
No |
|
The United States Pharmacopoeia standards relating to the safe storage and handling of drugs? |
Yes |
No |
|
The safe storage and handling of home medical devices? |
|
|
|
|
|
|
Yes |
No |
|
Prescription terminology, abbreviations, and format? |
|
|
|
|
|
|
|
|
|
|
Yes |
No |
For all of the above questions answered yes, you must submit appropriate proof to verify qualifications.
7.Certification of Exemptee - Please read carefully and sign below
I understand that falsification of the information on this form may constitute grounds for denial or revocation of the license. I hereby certify under penalty of perjury under the laws of the State of California to the truth and accuracy of all statements, answers and representations made in this application, including all supplementary statements. I also certify that I personally completed this application and have read and understand the instructions attached to this application.
Applicant Exemptee signature: (in full, no initials)
CDPH 8695 (09/09) |
Fund Code 3018 Index 5624 PCA 76223 Receipt Source 125700 Agency Source 49 |
Page 1 of 3 |
State of California—Health and Human Services Agency |
California Department of Public Health |
|
Food and Drug Branch |
THIS AREA IS TO BE COMPLETED BY THE EMPLOYER
8. Legal Name of Home Medical Device Retailer: |
|
|
|
HMDR license number: |
|
|
|
|
|
|
|
|
|
|
|
Business name: (if different) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Facility Address: |
Number and Street |
City |
|
State |
|
Zip Code |
|
|
|
|
9. The applicant medical device retailer will sell the following products: (Check all that apply) |
|
|
|
|
Respiratory Equipment / O2 Supplies |
Incontinence Supplies |
|
Walkers, Canes, Commodes |
|
|
|
CPAPS, BiPAPS |
|
Custom Wheelchairs |
|
Hospital Beds / Mattresses |
|
|
|
|
TENS Units |
|
Power Wheelchairs |
|
Other: Describe Below or attach list of products. |
|
|
Infusion Pumps |
|
Manual Wheelchairs |
|
___________________________________________________ |
|
Catheters |
|
Nutritional Supplements |
|
|
|
|
|
|
|
|
|
|
CPM Machines |
|
Diabetic Test Supplies |
|
___________________________________________________ |
|
|
|
|
10. |
Does this Home Medical Device Retailer currently employ the person whose name appears on this application? |
Yes |
No |
|
|
|
|
11. |
Will this person replace an Exemptee licensed by the California Department of Public Health? |
Yes |
No (Attach copy) |
|
Name of Exemptee being replaced : |
|
|
Exemptee Number: |
|
|
|
______________________________________________________________ |
___________________________ |
|
|
|
|
|
|
|
|
12. |
List business hours and days that the applicant will be working at this facility: |
|
|
|
|
|
____________________________ |
|
|
|
|
|
|
|
|
13. |
Enter other Exemptee license number(s) that applicant possesses: |
|
|
|
|
|
|
_______________________________ |
|
|
|
|
|
|
|
14. |
If applicant is working at various locations explain how facility intends to provide coverage in applicant’s absence: |
|
|
______________________________________________________________________________________________________________
(attach a separate sheet if necessary)
15.Certification of Employer – Read carefully and sign below
I hereby certify that the application completed on this form is being presented to the Food and Drug Branch with my knowledge and approval. Also, it is my understanding that a person certified by the Food and Drug Branch must be on the premises and actively supervising operations at all times when prescription devices are being dispensed. I certify under penalty of perjury under the laws of the State of California to the truth and accuracy of all statements, answers, and representations made in the foregoing application, including all supplementary statements.
16. Employer’s original signature: (in blue ink)
17. License Fee Due (Fee is Non Refundable) |
Enter Each Fee Below: |
|
|
|
|
License fee (see page 3) |
$ |
|
Late Fee ($10 if over 30 days late) |
$ |
|
Total Payment Due |
$ |
Make Checks Payable to: CALIFORNIA DEPARTMENT OF PUBLIC HEALTH See page 3 for mailing address
CDPH 8695 (09/09) |
Fund Code 3018 Index 5624 |
PCA 76223 Receipt Source 125700 Agency Source 49 |
Page 2 of 3 |
State of California—Health and Human Services Agency |
California Department of Public Health |
|
Food and Drug Branch |
Home Medical Device Retailer Exemptee License Application Instructions
Please complete and/or amend this application as is most appropriate to your facility. Include the appropriate fee for each application as indicated in the fee schedule and make check payable to: CA DEPARTMENT OF PUBLIC HEALTH. The application cannot be processed without the appropriate fees, complete documentation and appropriate signatures. Unsigned or incomplete applications cannot be processed and will be returned. The following are further instructions on how to complete this application:
1.Your Information: Your legal name as it is to appear on the license issued by the Department of Public Health. Residence address: Enter the number, street, city, state and Zip code for your residence. If this is a renewal, enter your current Exemptee license number.
2.Employer Information: The legal name of the Home Medical Device Retailer facility where you will be working. Address: Enter the number, street, city, state and Zip code for this facility.
3.Correspondent: Enter the name of the person to contact for information regarding this application and their title.
4.Mailing Address: This address is where licensing information is to be sent if the address is a different location than the Employer address.
5.Felony: Has the applicant ever been convicted of a felony? If “Yes,” provide an explanation on a separate sheet.
6.Minimum qualifications:
•Education: High school diploma GED or equivalent. Attach copies of any applicable certifications or licenses that you may hold.
•On-the-Job Training: Attach copies of current employer’s training records listing job-specific training provided and dates completed.
•Work Experience: One or more years paid experience, attach dates, name(s) of employer(s), and addresses. Training must have been supervised by a licensed exemptee, Pharmacist-In-Charge or equivalent.
•Training Programs: Indicate by yes or no the training you have completed specific to the five topics listed. Attach copies of certificates or transcripts.
7.Certification of Applicant: After reading the instruction paragraph your signature is needed, please sign in full (no initials) and date.
Numbers 8 through 16 are to be completed by the employer.
8.Name of Firm: Enter the full name of the business, HMDR license: Enter the current Home Medical Device Retailer facility license
number. Corporate Name: Name of corporation if different from HMDR name. Facility Address: Enter the number, street, city, state and Zip code for this facility location.
9.Products type: Place an (x) in the boxes that correctly describe products that this firm handles (check all that apply).
10.Current Employment: Check the appropriate box to verify employment.
11.Replacement of Licensed Exemptee: Check box: if applicant is replacing a licensed Exemptee. Name: Exemptee being replaced.
Certificate number: Exemptee being replaced certificate number. (Attach copy)
12.Enter business days and hours of application at facility.
13.Enter any other Home Medical Device Retailer Exemptee license numbers applicant possesses.
14.Provide explanation of Home Medical Device Retailer facility coverage in controlling prescription products when applicant is unavailable.
15.& 16. Certification of Employer: After reading the instruction paragraph the employer’s original signature is needed, please sign, state title of signatory and date the signature.
17.Payment
|
License Category |
Fee |
|
|
Interval |
|
Exemptee Application |
$250.00 |
|
|
New ( Never licensed as Exemptee with FDB) |
|
Fee / License fee |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Exemptee License Fee |
$150.00 |
|
|
Annual Renewal |
|
|
|
|
|
|
|
Exemptee License Fee |
$150.00 |
|
|
Additional license, Relocation, Change of Ownership |
|
|
|
|
|
|
**LICENSE FEES ARE NON-REFUNDABLE AND NON-TRANSFERABLE TO OTHER LOCATIONS OR ENTITIES
MAKE CHECKS PAYABLE TO: California Department of Public Health
MAIL APPLICATION AND CHECK TO:
California Department of Public Health
Food and Drug Branch - Cashier
P.O. Box 997435, MS-7602
Sacramento, CA 95899-7435
If you have any questions, please contact the Home Medical Device Retailer licensing desk at (916) 650-6500. You may also visit our internet web site at: http://www.cdph.ca.gov/programs/Pages/FDB.aspx for timely program news and a blank copy of this application form.
CDPH 8695 (09/09) |
Page 3 of 3 |