
To fill out the DSD/Instructor Application online, no additional software is needed. Open the FormsPal PDF editor in your browser, enter your information, and download or print the finished document for submission to the CDPH Licensing and Certification Program.
Steps to complete the form using the FormsPal editor
Step 1: Click the "Get Form" button above to open the PDF editor. The tool loads the form instantly in your browser with the full document visible.
Step 2: Use the editor to type in your information, adjust existing entries, and add your signature. The editor supports all fields in this document.
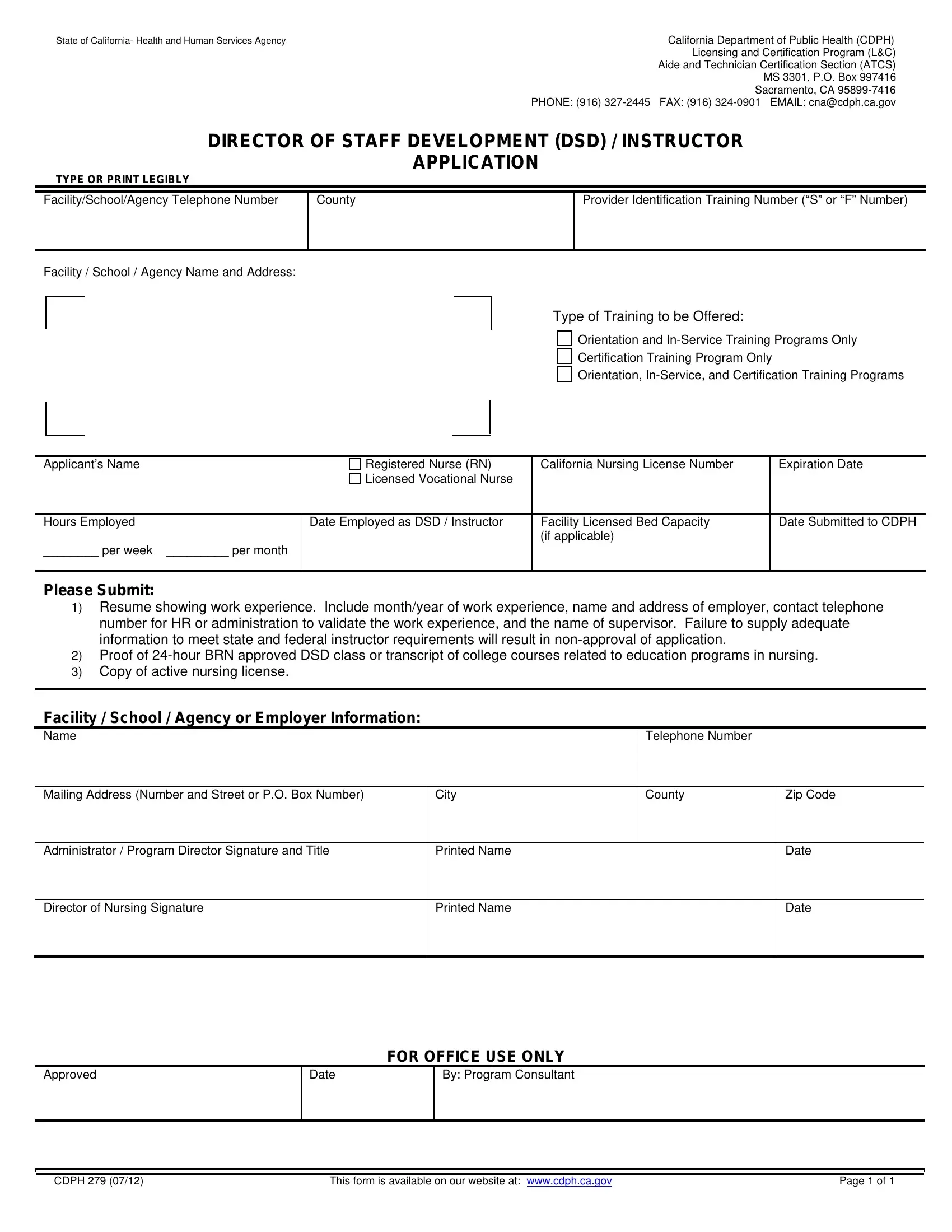
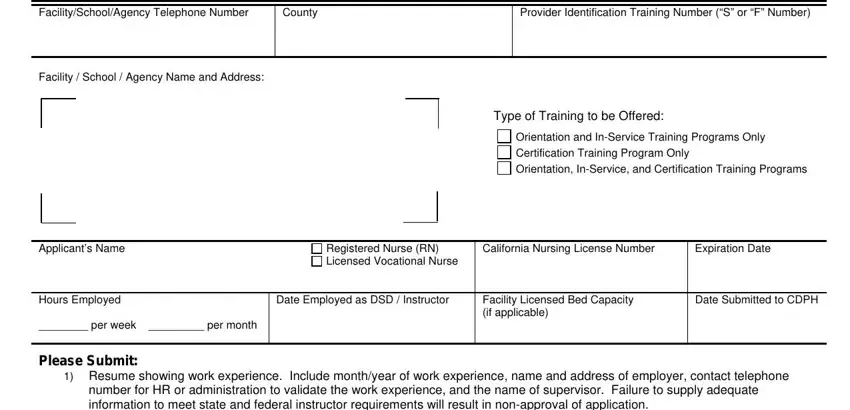
The DSD form includes the following fields to complete:
1. Begin by filling in all required applicant information in the first section. Review each field carefully before moving to the next.
2. In the second section, enter details for these fields: Facility, School, or Agency; Telephone Number; Mailing Address, City, County, and Zip Code; Administrator or Program Director name; Director of Nursing Signature; Printed Name; Date; and the FOR OFFICE USE ONLY section.
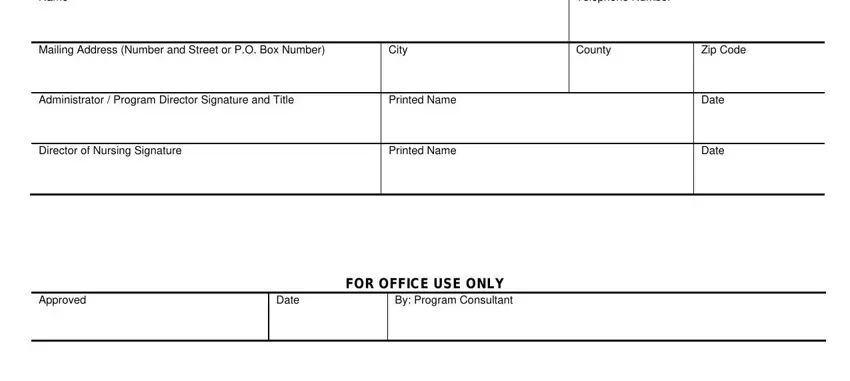
The Printed Name field in section 2 is a common area for errors. Double-check your entry before saving.
Step 3: Click "Done" to finalize the form. Download the completed document as a PDF, then mail your full packet to the CDPH Licensing and Certification Program for review.
Related CDPH forms for DSD and Instructor applicants
Depending on your facility and role, you may also need to submit these related California Department of Public Health forms:
Common questions about the DSD application process
Who needs to submit Form 279? Any RN or LVN in California who wants to provide orientation, in-service training, or certification programs at a licensed healthcare facility must receive DSD or Instructor approval from CDPH before beginning those duties.
What happens if my packet is incomplete? CDPH will not approve incomplete applications. Include all required credentials, employment history, educational background, and signatures before submitting your packet.
Can I complete the form online? Yes. Use the FormsPal editor above to fill in and download the form. Print the finished document and include it in your mailed application packet to CDPH.