
Form Cdph 8695 can be filled in very easily. Just make use of FormsPal PDF editor to complete the job without delay. The editor is continually improved by our staff, receiving handy features and becoming better. Here is what you will have to do to get started:
Step 1: Open the PDF form inside our tool by pressing the "Get Form Button" at the top of this page.
Step 2: With the help of this handy PDF editor, it is possible to do more than just fill out blank form fields. Try all of the functions and make your docs appear faultless with custom text put in, or modify the original content to excellence - all that backed up by an ability to incorporate almost any pictures and sign the document off.
This document needs some specific details; to guarantee accuracy, be sure to heed the subsequent suggestions:
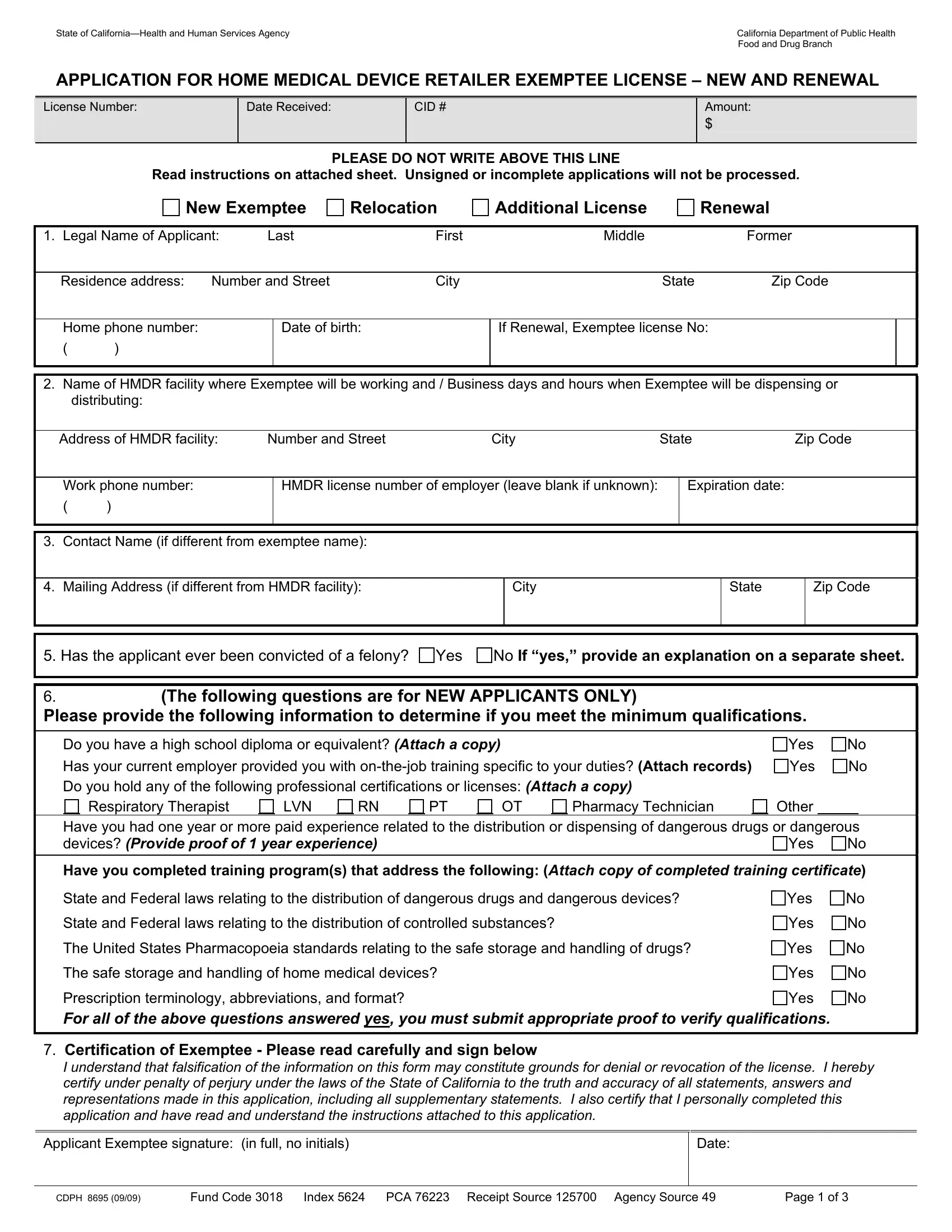
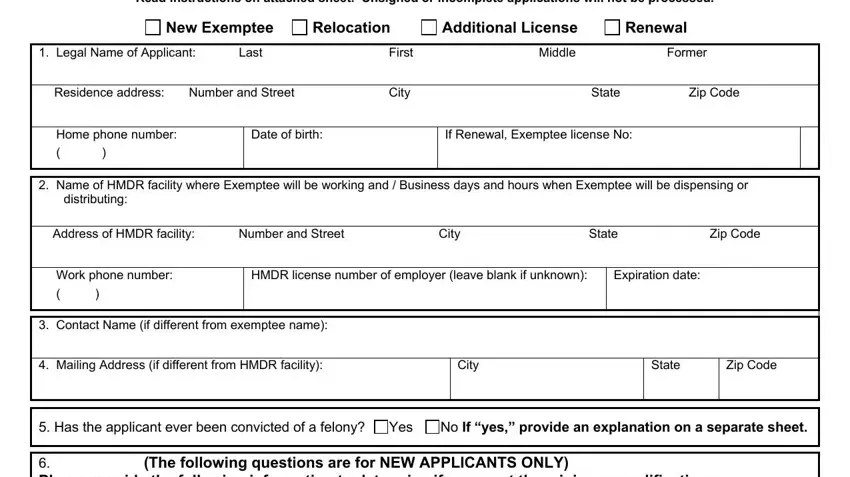
1. The Form Cdph 8695 will require particular information to be typed in. Be sure the following blanks are filled out:
2. Once this array of fields is completed, it's time to add the required specifics in The following questions are for, Yes No Do you have a high school, Respiratory Therapist, Other Have you had one year or, Pharmacy Technician, LVN, Have you completed training, State and Federal laws relating to, State and Federal laws relating to, The United States Pharmacopoeia, The safe storage and handling of, Yes No, Yes No, Yes No, and Yes No so you're able to progress further.
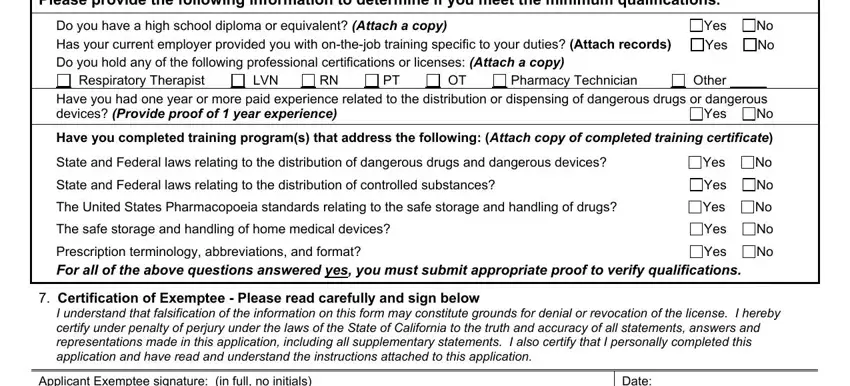
3. This third segment is normally rather easy, Applicant Exemptee signature in, Date, and CDPH Fund Code Index PCA - every one of these form fields must be completed here.

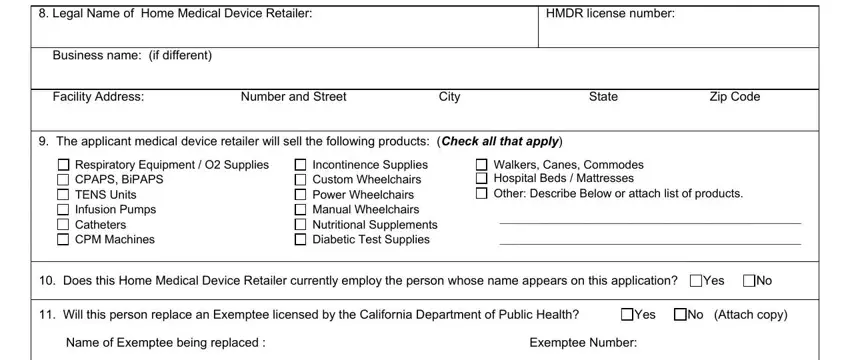
4. Filling out Legal Name of Home Medical Device, Business name if different, HMDR license number, Facility Address The applicant, Number and Street, City, State, Zip Code, Respiratory Equipment O Supplies, Incontinence Supplies Custom, Walkers Canes Commodes Hospital, Does this Home Medical Device, Yes No, Will this person replace an, and Name of Exemptee being replaced is vital in the fourth form section - always take your time and fill in every blank!
5. To wrap up your form, this final section has a number of additional fields. Completing List business hours and days that, Enter other Exemptee license, If applicant is working at, attach a separate sheet if, Certification of Employer Read, I hereby certify that the, Employers original signature in, Title of person signing, and Date should wrap up everything and you're going to be done quickly!
Those who use this form often make some errors while filling in Employers original signature in in this area. You should re-examine everything you type in right here.
Step 3: Always make sure that your details are right and just click "Done" to conclude the process. Right after setting up afree trial account with us, you will be able to download Form Cdph 8695 or email it at once. The PDF file will also be easily accessible through your personal account with all your modifications. FormsPal is focused on the confidentiality of our users; we make certain that all personal data put into our editor is protected.