
Handling PDF files online is certainly easy using our PDF tool. Anyone can fill out Form Cf 377 2A here without trouble. Our editor is constantly evolving to provide the very best user experience achievable, and that is thanks to our commitment to continuous enhancement and listening closely to customer comments. This is what you'd want to do to begin:
Step 1: Firstly, open the pdf tool by clicking the "Get Form Button" at the top of this page.
Step 2: This editor will allow you to change most PDF documents in a variety of ways. Enhance it by writing your own text, correct what's already in the PDF, and include a signature - all when you need it!
This PDF form will require specific information to be entered, therefore be sure you take the time to enter what's asked:
1. Fill out your Form Cf 377 2A with a group of major fields. Get all of the required information and make sure there's nothing forgotten!
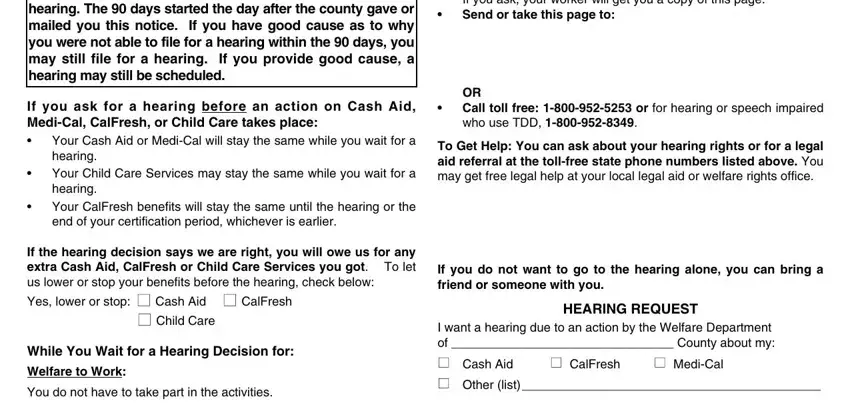
2. The third step is to complete the next few fields: If you ask your worker will get, OR Call toll free or for hearing, To Get Help You can ask about your, If you do not want to go to the, HEARING REQUEST, I want a hearing due to an action, n CalFresh n MediCal, You have the right to ask for a, If you ask for a hearing before an, Your Cash Aid or MediCal will stay, If the hearing decision says we, Child Care, While You Wait for a Hearing, Welfare to Work, and You do not have to take part in.
3. Within this step, take a look at Heres Why, n If you need more space check, n I need the state to provide me, A relative or friend cannot, My language or dialect is, NAME OF PERSON WHOSE BENEFITS WERE, BIRTH DATE, STREET ADDRESS, PHONE NUMBER, STATE, ZIP CODE, DATE, You may receive child care, If we told you your other, and If we told you we will pay your. All of these need to be filled in with greatest focus on detail.
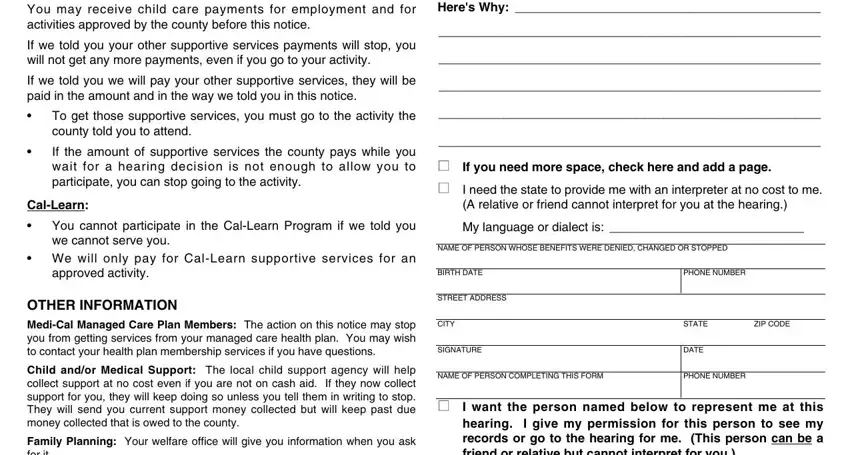
4. The following section will require your information in the following areas: Family Planning Your welfare, n I want the person named below to, Hearing File If you ask for a, NAME, STREET ADDRESS, CITY, NA BACK REPLACES NA BACK AND EP, PHONE NUMBER, STATE, and ZIP CODE. Remember to fill out all of the needed details to go forward.

As for STATE and Hearing File If you ask for a, be certain you review things in this current part. The two of these are the most important fields in this form.
Step 3: Before submitting your form, make certain that all blank fields were filled out right. The moment you believe it's all good, click “Done." Obtain your Form Cf 377 2A once you sign up at FormsPal for a free trial. Instantly get access to the document from your FormsPal account, along with any modifications and changes being all synced! FormsPal is devoted to the personal privacy of all our users; we make certain that all information coming through our tool continues to be secure.