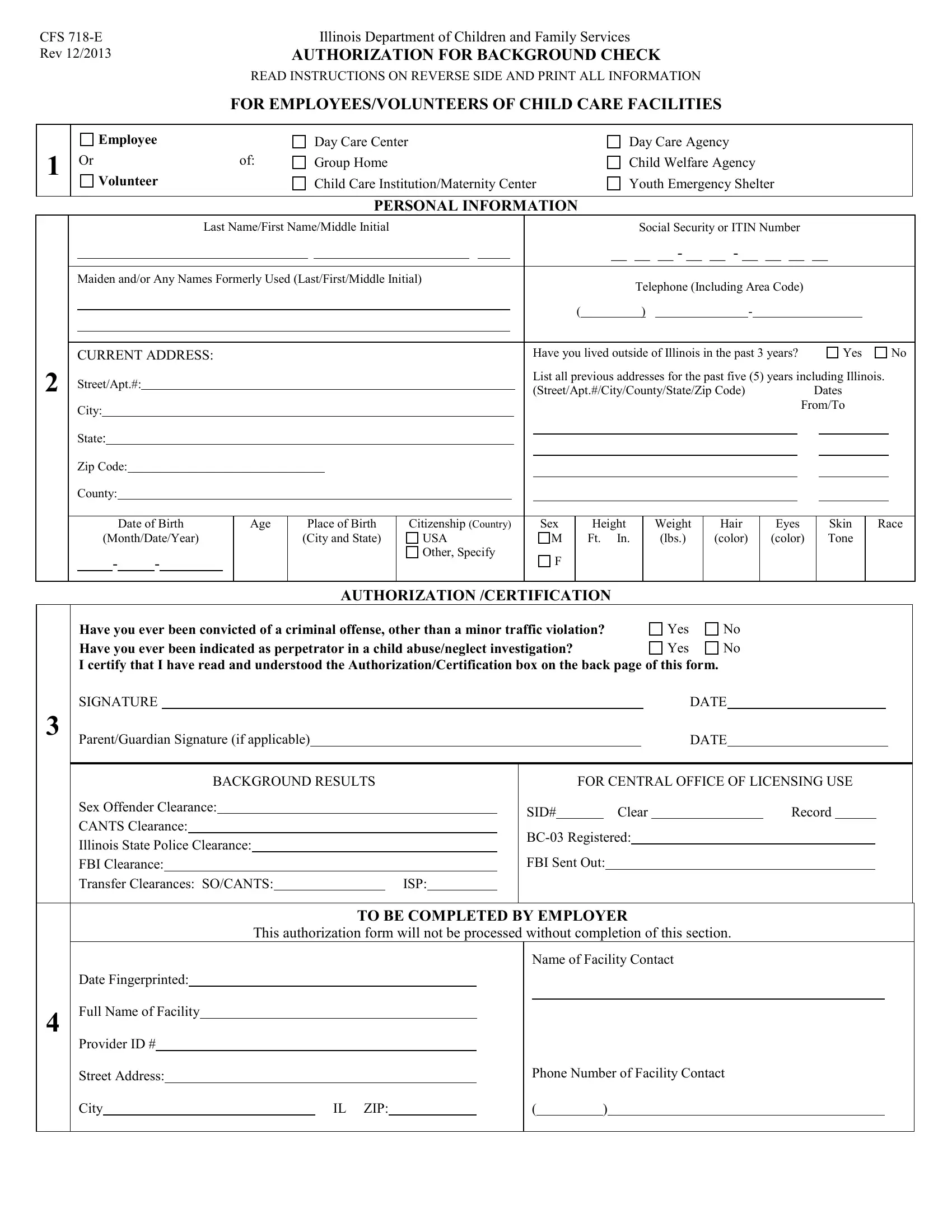
Ensuring the safety and well-being of children in care facilities is of paramount importance, making thorough background checks an essential component of the hiring process. The CFS 718-E form, developed by the Illinois Department of Children and Family Services and revised in December 2013, serves this critical function. Required for employees and volunteers, aged 13 or older, working in a variety of child care settings, this form facilitates a comprehensive evaluation of an individual's eligibility through a meticulous review of their criminal history, involvement in child abuse/neglect investigations, and other pertinent personal information. The process involves the collection of detailed personal data, including past residences and any aliases, alongside explicit consent for the Illinois Department of Children and Family Services to conduct criminal and child abuse checks. Moreover, the form mandates the disclosure of any past criminal offenses and instances of being indicated as a perpetrator in child abuse or neglect cases, ensuring a thorough assessment of potential risks. Employers play a crucial role in this process, required to verify the completeness and accuracy of the information provided before proceeding with fingerprinting. This form not only ensures the safety of children but also aids in the maintenance of a secure environment within Illinois child care facilities. Importantly, individuals have the right to contest any discrepancies found in their records, as indicated by the form's instructions, underscoring the process's fairness and transparency. The CFS 718-E form, therefore, stands as a vital tool in safeguarding vulnerable populations and upholding the standards of care expected by the community.
| Question | Answer |
|---|---|
| Form Name | Form Cfs 718E |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CANTS, CFS, printable exemption page for chapter 7 champaign il, ISP |
CFS |
|
Illinois Department of Children and Family Services |
|||
Rev 12/2013 |
|
AUTHORIZATION FOR BACKGROUND CHECK |
|||
|
|
READ INSTRUCTIONS ON REVERSE SIDE AND PRINT ALL INFORMATION |
|||
|
|
FOR EMPLOYEES/VOLUNTEERS OF CHILD CARE FACILITIES |
|||
|
|
|
|
|
|
1 |
Employee |
|
Day Care Center |
Day Care Agency |
|
Or |
of: |
Group Home |
Child Welfare Agency |
||
|
|||||
|
Volunteer |
|
Child Care Institution/Maternity Center |
Youth Emergency Shelter |
|
|
|
|
|
|
|
PERSONAL INFORMATION
2
|
|
|
|
|
|
|
|
|
|
|
Last Name/First Name/Middle Initial |
|
|
|
|
|
|
|
|
|
|
Social Security or ITIN Number |
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__ __ __ - __ __ - __ __ __ __ |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Maiden and/or Any Names Formerly Used (Last/First/Middle Initial) |
|
|
|
|
|
Telephone (Including Area Code) |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
|
) |
|
|
- |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
CURRENT ADDRESS: |
|
|
|
|
|
|
|
|
|
|
|
Have you lived outside of Illinois in the past 3 years? |
|
Yes |
|
|
No |
|||||||||||||||||||||||
Street/Apt.#: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
List all previous addresses for the past five (5) years including Illinois. |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Street/Apt.#/City/County/State/Zip Code) |
|
|
|
|
Dates |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From/To |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
State: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Zip Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
County: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
Date of Birth |
|
|
Age |
Place of Birth |
Citizenship (Country) |
|
|
Sex |
|
Height |
|
Weight |
Hair |
|
|
Eyes |
|
Skin |
|
Race |
|||||||||||||||
|
|
(Month/Date/Year) |
|
|
|
(City and State) |
USA |
|
|
M |
|
Ft. In. |
|
|
(lbs.) |
(color) |
|
|
(color) |
|
Tone |
|
|
|
||||||||||||||||
- |
|
|
- |
|
|
|
|
|
|
|
Other, Specify |
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AUTHORIZATION /CERTIFICATION
3
Have you ever been convicted of a criminal offense, other than a minor traffic violation? |
Yes |
No |
Have you ever been indicated as perpetrator in a child abuse/neglect investigation? |
Yes |
No |
I certify that I have read and understood the Authorization/Certification box on the back page of this form.
SIGNATURE |
|
DATE |
||
Parent/Guardian Signature (if applicable) |
|
|
DATE |
|
BACKGROUND RESULTS
Sex Offender Clearance:
CANTS Clearance:
Illinois State Police Clearance:
FBI Clearance:
Transfer Clearances: SO/CANTS: |
|
ISP: |
|
|
|
|
|
FOR CENTRAL OFFICE OF LICENSING USE
SID# ClearRecord
FBI Sent Out:
4
TO BE COMPLETED BY EMPLOYER
This authorization form will not be processed without completion of this section.
Name of Facility Contact
Date Fingerprinted:
Full Name of Facility
Provider ID #
Street Address: |
|
Phone Number of Facility Contact |
City |
|
IL ZIP: |
|
|
|
|
|
()
INSTRUCTIONS FOR COMPLETION OF
CFS
WHO SHOULD USE THIS FORM: This form must be completed by employees and volunteers, age 13 or older, who work in a day care center, day care agency, group home, child welfare agency, child care institution/maternity center or youth emergency shelter. Employees of day care homes, foster care homes and group day care homes are to use form CFS 718. The Parent or Guardian’s signature is required if background check is for a minor.
Do not send a request for a Child Abuse/Neglect Tracking System (CANTS)
check to Central Licensing until the person has been fingerprinted.
SECTIONS 1, 2 AND 3
Employer must instruct every person subject to a background check to complete the first three sections identifying the type of facility and what role they will have at the facility and all personal information. All identifying information must be accurate and complete.
PRINT ALL INFORMATION
Name:
Social Security or ITIN No.
Address:
Race:
Current and all former names used by the individual must be included. If no other names, write “none.”
THIS FORM WILL NOT BE PROCESSED WITHOUT A COMPLETE SOCIAL SECURITY OR INDIVIDUAL TAXPAYER IDENTIFICATION (ITIN) NUMBER
Current and all addresses, including county, where the person has lived in the past five years (If outside of Illinois, check appropriate box)
Enter all codes that apply
BL/AA |
Black or African American |
ASIAN |
Asian |
HISP ORG |
Indicate whether the individual is of Hispanic origin |
NH/PI |
Native Hawaiian or Other Pacific Islander |
WHITE |
White |
UNDET |
Undetermined |
AI/AN |
American Indian or Alaskan Native |
|
|
Each Person “must” answer the questions “Have you ever been convicted of a criminal offense, other than minor traffic violation?”
The person completing the identification information must sign and date page 1 of the authorization form.
SECTION 4 - EMPLOYER
The Authorization for Background Check must be submitted to the employer for completion of Section 4 and to check the form for completeness and accuracy before the employee is fingerprinted.
Employer must complete the following:
Name of Facility |
Name of facility where employed. Use the full name which appears on the license application or the license. |
|
(DO NOT USE ACRONYMS) |
Street/City/Zip |
The site of licensed facility where person is employed. |
Provider ID # |
The Provider ID # is required. (The number which appears on the license certificate for the facility.) |
AUTHORIZATION/CERTIFICATION
I authorize the Illinois Department of Children and Family Services to conduct an investigation to determine whether I have ever been charged with a crime and, if so, the disposition of those charges. I authorize the Department to request information and assistance from the U.S. Justice Department and the Illinois Department of Law Enforcement in the conduct of this investigation. I authorize the Department to periodically search the Child Abuse and Neglect Tracking System to determine whether I have been a perpetrator of an “indicated” incident of child abuse or neglect pursuant to the Abused and Neglected Child Reporting Act. The child abuse and neglect background check and the criminal history investigation may be used for considering an application for license, current or prospective employment, or service as a volunteer in a child care facility. Persons
I understand that information obtained as a result of my authorizing this investigation is confidential but may be shared with my employer, prospective employer or with authorized licensing staff in accordance with applicable state and federal law and DCFS Regulations. I further certify that the information provided on this form is true and correct. I acknowledge that falsification of any information provided above and/or the results of the background check may be full and sufficient grounds to deny the application for licensure or may result in the termination of my employment.
Should you feel that the information on your Illinois State Police record or Federal Bureau of Investigation record is incorrect you may visit: http://www.ilga.gov/commission/jcar/admincode/020/02001210sections.html for the ISP and http://www.fbi.gov for FBI.