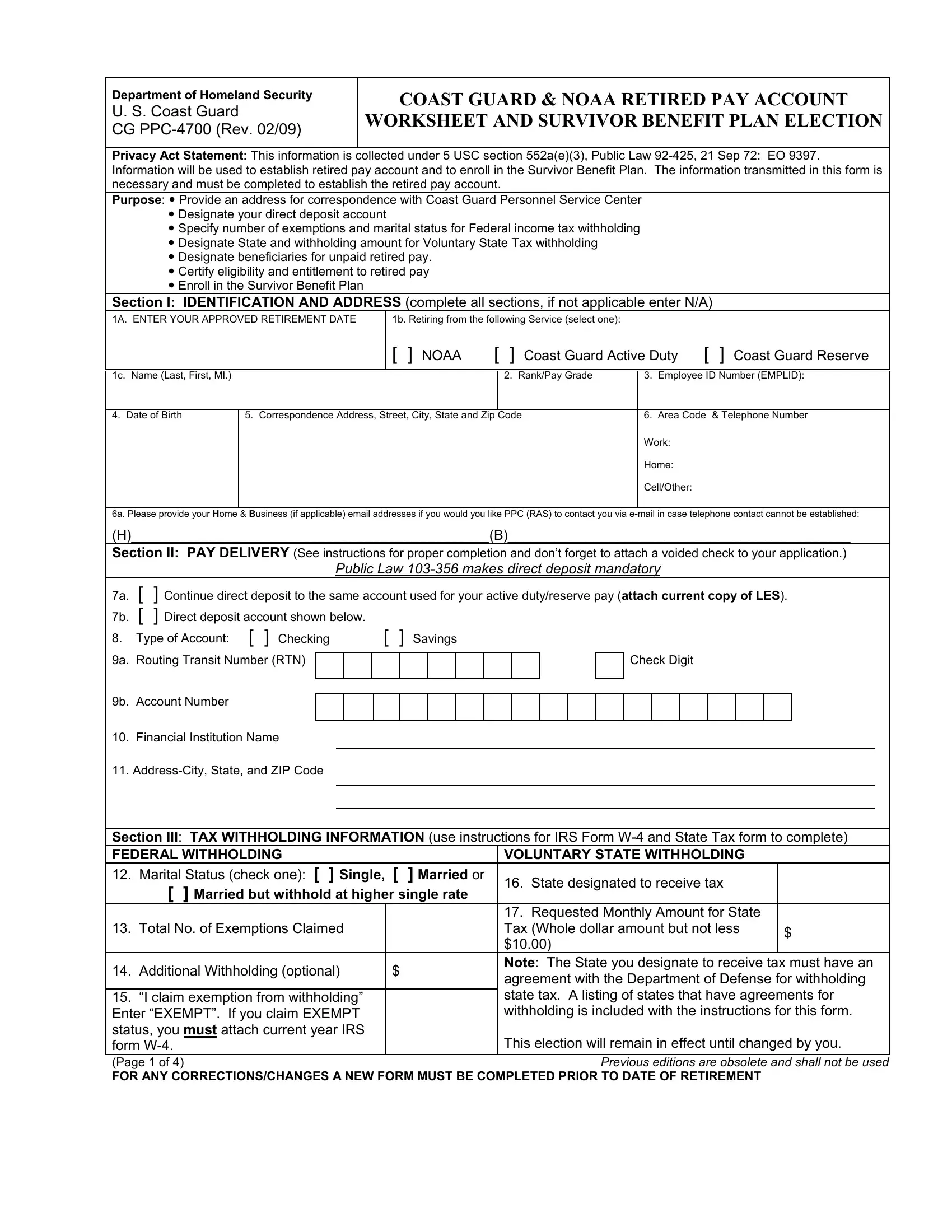
Embarking on retirement from the U.S. Coast Guard or NOAA requires careful planning and considerable paperwork, one critical piece being the CG PPC-4700 form. As per the Department of Homeland Security's regulations, this form serves a multifaceted function, crucial for setting the stage for a smooth transition into retirement. It addresses the establishment of a retired pay account, directly linking to the retiree's financial readiness. Moreover, the form plays a pivotal role in enrolling members in the Survivor Benefit Plan (SBP), ensuring that beneficiaries are aptly protected. The CG PPC-4700 form requests detailed personal information for identification and tax purposes, pays delivery instructions to facilitate the direct deposit of benefits, and guidelines for federal and state tax withholdings. Additionally, it encompasses a section devoted to the designation of beneficiaries for unpaid retired pay, underscoring its comprehensive nature in safeguarding the retiree's financial interests post-service. Completing this form accurately is paramount, as it encompasses not only the certification data crucial for the payment of retired personnel but also enlists an election section for the Survivor Benefit Plan, highlighting choices that could significantly impact the retiree's family's financial future. Navigating through this form requires a thorough understanding of its sections and implications, making it an indispensable step towards securing a financially stable retirement.
| Question | Answer |
|---|---|
| Form Name | Form Cg Ppc 4700 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | W-4, SSN, cg ppc 4700, NOAA |
