Encompassing both the framework for engaging with judicial proceedings and the integration of accessibility rights, the Clk Ct 914 form serves as a crucial element within the legal landscape of Miami-Dade County, Florida. Designed to provide an efficient pathway for defendants to waive the traditional service of process, this document facilitates a smoother initiation of legal actions by encouraging the use of mail services for the delivery of lawsuit notifications. By offering defendants the option to acknowledge receipt of a lawsuit without necessitating formal service by a process server, the form not only streamlines procedural requirements but also embodies a cost-saving measure for all parties involved. The inclusion of explicit instructions for defendants—or their representatives—to retain defenses or objections except those related to summons defects underscores the form's emphasis on legal fairness and procedural clarity. Moreover, the form embodies the judiciary's commitment to inclusivity through its adherence to the Americans with Disabilities Act of 1990 (ADA), ensuring that individuals with disabilities receive the necessary accommodations to participate in legal processes fully. This consideration highlights the broader duty of the court system to ensure equal access and participation for all individuals, reflecting a multifaceted approach to legal proceedings within Miami-Dade County's judicial framework.
| Question | Answer |
|---|---|
| Form Name | Form Clk Ct 914 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | waiver of service of process form florida, return, in, of |
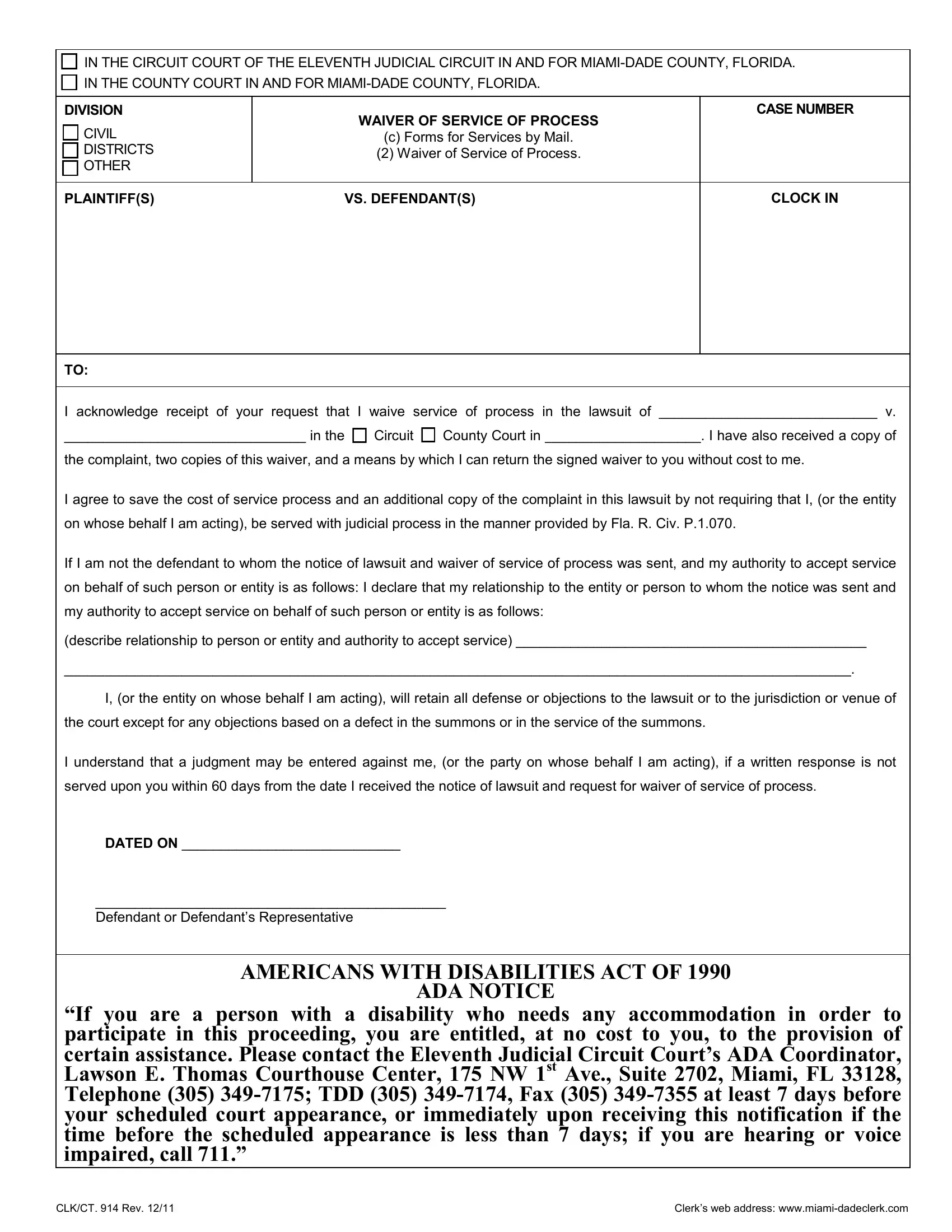
IN THE CIRCUIT COURT OF THE ELEVENTH JUDICIAL CIRCUIT IN AND FOR
IN THE COUNTY COURT IN AND FOR
DIVISION
CIVIL
DISTRICTS
OTHER
WAIVER OF SERVICE OF PROCESS
(c)Forms for Services by Mail.
(2)Waiver of Service of Process.
CASE NUMBER
PLAINTIFF(S) |
VS. DEFENDANT(S) |
CLOCK IN
TO:
I acknowledge receipt of your request that I waive service of process in the lawsuit of ____________________________ v.
_______________________________ in the Circuit County Court in ____________________. I have also received a copy of
the complaint, two copies of this waiver, and a means by which I can return the signed waiver to you without cost to me.
I agree to save the cost of service process and an additional copy of the complaint in this lawsuit by not requiring that I, (or the entity on whose behalf I am acting), be served with judicial process in the manner provided by Fla. R. Civ. P.1.070.
If I am not the defendant to whom the notice of lawsuit and waiver of service of process was sent, and my authority to accept service on behalf of such person or entity is as follows: I declare that my relationship to the entity or person to whom the notice was sent and my authority to accept service on behalf of such person or entity is as follows:
(describe relationship to person or entity and authority to accept service) _____________________________________________
_____________________________________________________________________________________________________.
I, (or the entity on whose behalf I am acting), will retain all defense or objections to the lawsuit or to the jurisdiction or venue of the court except for any objections based on a defect in the summons or in the service of the summons.
I understand that a judgment may be entered against me, (or the party on whose behalf I am acting), if a written response is not served upon you within 60 days from the date I received the notice of lawsuit and request for waiver of service of process.
DATED ON ____________________________
_____________________________________________
Defendant or Defendant’s Representative
AMERICANS WITH DISABILITIES ACT OF 1990
ADA NOTICE
“If you are a person with a disability who needs any accommodation in order to participate in this proceeding, you are entitled, at no cost to you, to the provision of certain assistance. Please contact the Eleventh Judicial Circuit Court’s ADA Coordinator, Lawson E. Thomas Courthouse Center, 175 NW 1st Ave., Suite 2702, Miami, FL 33128, Telephone (305)
CLK/CT. 914 Rev. 12/11 |
Clerk’s web address: |