

With the online tool for PDF editing by FormsPal, it is easy to fill in or alter Form Cmd 1014A Forpf right here and now. Our tool is continually developing to give the best user experience achievable, and that's because of our resolve for continual improvement and listening closely to user feedback. Should you be seeking to begin, here is what it's going to take:
Step 1: Access the PDF file inside our editor by hitting the "Get Form Button" in the top part of this page.
Step 2: With our state-of-the-art PDF editor, you can actually accomplish more than simply fill out blanks. Express yourself and make your documents seem high-quality with custom text incorporated, or tweak the file's original content to perfection - all that comes along with an ability to add any kind of pictures and sign it off.
This PDF form will require particular info to be filled in, hence make sure to take some time to type in what's expected:
1. Whenever filling out the Form Cmd 1014A Forpf, be sure to incorporate all necessary blank fields within the associated area. This will help facilitate the work, enabling your details to be processed fast and accurately.
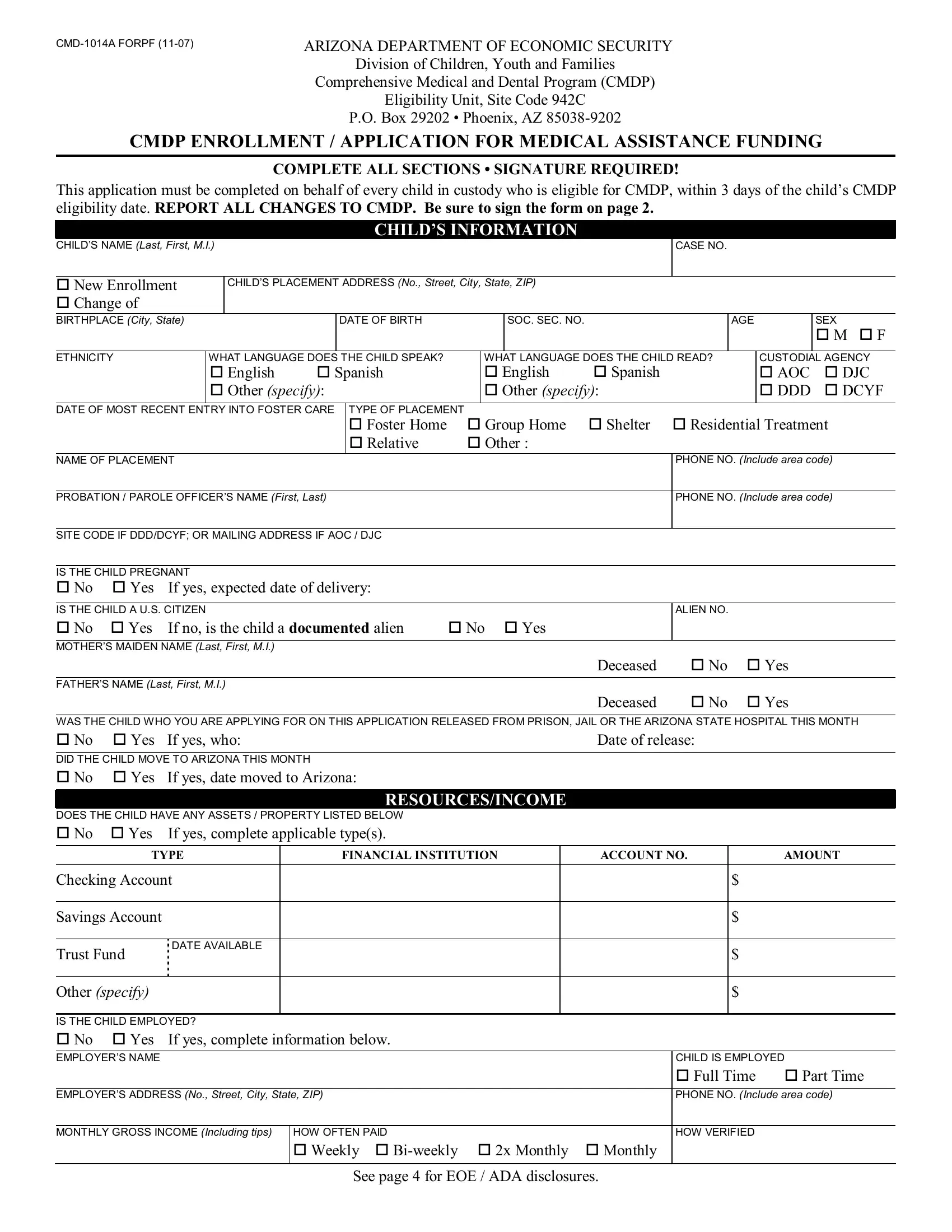
2. Soon after the previous section is done, go on to enter the relevant details in these - IS THE CHILD A US CITIZEN cid No, Deceased cid No cid Yes, Date of release, DOES THE CHILD HAVE ANY ASSETS, If yes complete applicable types, RESOURCESINCOME, TYPE, FINANCIAL INSTITUTION, ACCOUNT NO, AMOUNT, Checking Account, Savings Account, Trust Fund, DATE AVAILABLE, and Other specify.
Many people frequently make errors while filling out TYPE in this section. You should definitely read again what you enter right here.
3. In this stage, take a look at IS THE CHILD SELFEMPLOYED cid No, TYPE OF BUSINESS, HOURS PER WEEK MONTHLY GROSS INCOME, MONTHLY EXPENSES, HOW VERIFIED, IS THE CHILD A STUDENT REGISTERED, If yes CHILD is a cid Full Time, If yes complete the applicable, Student, HOW VERIFIED, TYPE, MONTHLY AMOUNT, Child Support, Social Security, and Parental Assessment. All of these have to be filled in with greatest accuracy.
4. It is time to proceed to this fourth part! Here you will get these PHONE NO Include area code, POLICY NO, EFFECTIVE DATE, DATE ENDED, DOES THE CHILD LISTED ON THIS, If yes specify needs, IS THERE A COURT ORDER FOR A, If yes specify, DOES THE CHILD HAVE A CURRENT, If yes specify illness, DOES THE CHILD LISTED ON THIS, If yes specify condition, VERY IMPORTANT SIGNATURE REQUIRED, CMDP needs your signature to, and Statement of Truth I swear under empty form fields to complete.
Step 3: Right after you've reviewed the information in the blanks, just click "Done" to finalize your document generation. Create a free trial plan with us and get direct access to Form Cmd 1014A Forpf - readily available in your personal account. FormsPal is focused on the confidentiality of our users; we ensure that all personal information coming through our tool is secure.