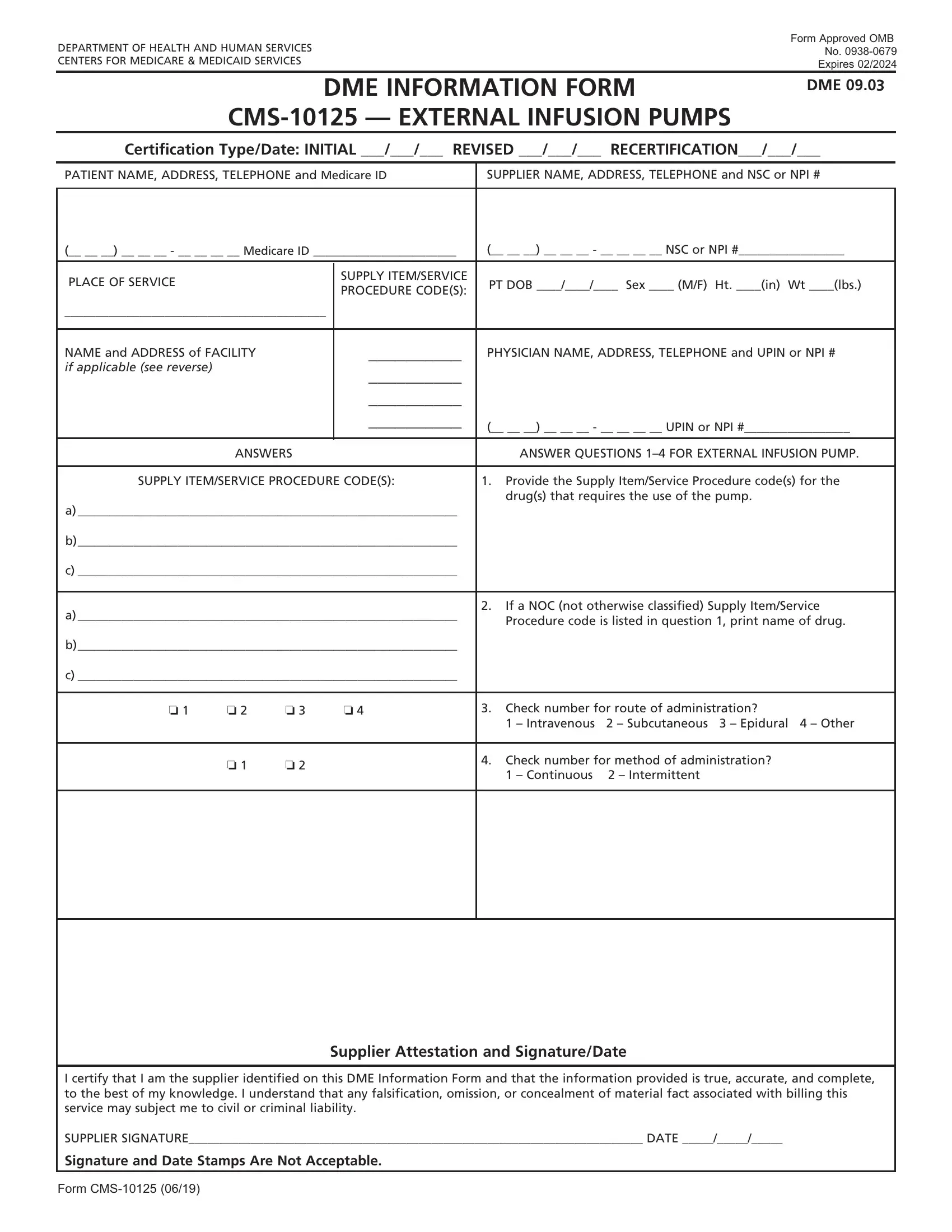
The CMS-10125 form, fundamentally designed by the Department of Health and Human Services and approved by the Office of Management and Budget (OMB No. 0938-0679), serves the crucial purpose of facilitating the provision of External Infusion Pumps under the Centers for Medicare & Medicaid Services. With an expiration date set for February 2024, this Durable Medical Equipment (DME) Information Form is integral for certifying initial, revised, or recertified claims for service. The form encapsulates various segments requiring detailed patient information, supplier data, and specific guidelines to accurately code the supply item/service procedure. Furthermore, it delineates a section dedicated to the physician's details, including their name, address, telephone number, and UPIN or NPI number if applicable. Questions aimed at unearthing clinical specifics about the item or service billed are a part of this comprehensive form, which also insists on a supplier attestation to validate the authenticity and accuracy of the information provided. Ultimately, the CMS-10125 form is pivotal in ensuring that the administration and billing of external infusion pumps are handled in a structured and standardized manner, safeguarding the alignment with regulatory compliance and aiding in the streamlined processing of Medicare claims.
| Question | Answer |
|---|---|
| Form Name | Form Cms 10125 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dif form sample, form recertification cms, cms dme forms print, form recertification cms online |
DEPARTMENT OF HEALTH AND HUMAN SERVICES |
Form Approved OMB |
No. |
|
CENTERS FOR MEDICARE & MEDICAID SERVICES |
Expires 02/2024 |
DME INFORMATION FORM
DME 09.03
Certification Type/Date: INITIAL ___/___/___ REVISED ___/___/___ RECERTIFICATION___/___/___
PATIENT NAME, ADDRESS, TELEPHONE and Medicare ID |
SUPPLIER NAME, ADDRESS, TELEPHONE and NSC or NPI # |
||||||
|
|
|
|||||
(__ __ __) __ __ __ - __ __ __ __ Medicare ID _______________________ |
(__ __ __) __ __ __ - __ __ __ __ NSC or NPI #_________________ |
||||||
|
|
|
|
|
|
|
|
PLACE OF SERVICE |
|
|
SUPPLY ITEM/SERVICE |
PT DOB ____/____/____ Sex ____ (M/F) |
Ht. ____(in) Wt ____(lbs.) |
||
|
|
PROCEDURE CODE(S): |
|||||
|
|
|
|
|
|
|
|
__________________________________________ |
|
|
|
|
|
||
|
|
|
|
||||
NAME and ADDRESS of FACILITY |
|
__________ |
PHYSICIAN NAME, ADDRESS, TELEPHONE and UPIN or NPI # |
||||
if applicable (see reverse) |
|
|
__________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__________ |
|
|
|
|
|
|
|
__________ |
(__ __ __) __ __ __ - __ __ __ __ UPIN or NPI #_________________ |
|||
|
|
|
|
||||
|
|
|
|
|
|||
|
ANSWERS |
|
|
ANSWER QUESTIONS |
|||
|
|
|
|||||
SUPPLY ITEM/SERVICE PROCEDURE CODE(S): |
1. Provide the Supply Item/Service Procedure code(s) for the |
||||||
|
|
|
|
|
drug(s) that requires the use of the pump. |
||
a) _____________________________________________________________ |
|
|
|
|
|||
b)_____________________________________________________________ |
|
|
|
|
|||
c) _____________________________________________________________ |
|
|
|
|
|||
|
|
|
|
|
|
||
a) _____________________________________________________________ |
2. |
If a NOC (not otherwise classified) Supply Item/Service |
|||||
|
Procedure code is listed in question 1, print name of drug. |
||||||
|
|
|
|
|
|||
b)_____________________________________________________________ |
|
|
|
|
|||
c) _____________________________________________________________ |
|
|
|
|
|||
|
|
|
|
|
|||
o 1 |
o 2 |
o 3 |
o 4 |
3. Check number for route of administration? |
|||
|
|
|
|
|
1 – Intravenous |
2 – Subcutaneous |
3 – Epidural 4 – Other |
|
|
|
|
|
|
||
|
o 1 |
o 2 |
|
4. |
Check number for method of administration? |
||
|
|
|
1 – Continuous |
2 – Intermittent |
|
||
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Supplier Attestation and Signature/Date
I certify that I am the supplier identified on this DME Information Form and that the information provided is true, accurate, and complete, to the best of my knowledge. I understand that any falsification, omission, or concealment of material fact associated with billing this service may subject me to civil or criminal liability.
SUPPLIER SIGNATURE_________________________________________________________________________ DATE _____/_____/_____
Signature and Date Stamps Are Not Acceptable.
Form

INSTRUCTIONS FOR COMPLETING DME INFORMATION FORM
FOR EXTERNAL INFUSION PUMPS
CERTIFICATION |
If this is an initial certification for this patient, indicate this by placing date (MM/DD/YY) needed |
TYPE/DATE: |
initially in the space marked “INITIAL.” If this is a revised certification (to be completed when |
|
the physician changes the order, based on the patient’s changing clinical needs), indicate the |
|
initial date needed in the space marked “INITIAL,” and also indicate the revision date in the |
|
space marked “REVISED.” If this is a recertification, indicate the initial date needed in the |
|
space marked “INITIAL,” and also indicate the recertification date in the space marked |
|
“RECERTIFICATION.” Whether submitting a REVISED or a RECERTIFICATION DIF, be sure to always |
|
furnish the INITIAL date as well as the REVISED or RECERTIFICATION date. |
PATIENT |
Indicate the patient’s name, permanent legal address, telephone number and his/her Medicare ID |
INFORMATION: |
as it appears on his/her Medicare card and on the claim form. |
SUPPLIER |
Indicate the name of your company (supplier name), address and telephone number along with |
INFORMATION: |
the Medicare Supplier Number assigned to you by the National Supplier Clearinghouse (NSC) |
|
or applicable National Provider Identifier (NPI). If using the NPI Number, indicate this by using |
|
the qualifier XX followed by the |
|
use the qualifier 1C followed by the |
PLACE OF SERVICE: |
Indicate the place in which the item is being used, i.e., patient’s home is 12, skilled nursing |
|
facility (SNF) is 31, End Stage Renal Disease (ESRD) facility is 65, etc. Refer to the DMERC |
|
supplier manual for a complete list. |
FACILITY NAME: |
If the place of service is a facility, indicate the name and complete address of the facility. |
SUPPLY ITEM/SERVICE List all HCPCS procedure codes for items ordered that require a DIF. Procedure codes that do PROCEDURE CODES: not require certification should not be listed in this section of the DIF.
PATIENT DOB, |
Indicate patient’s date of birth (MM/DD/YY) and sex (male or female); height in inches |
HEIGHT, WEIGHT |
and weight in pounds, if required. |
AND SEX: |
|
PHYSICIAN NAME, |
Indicate the physician’s name and complete mailing address. |
ADDRESS: |
|
PHYSICIAN |
Accurately indicate the treating physician’s Unique Physician Identification Number (UPIN) or |
INFORMATION: |
applicable National Provider Identifier (NPI). If using the NPI Number, indicate this by using the |
|
qualifier XX followed by the |
|
by the |
PHYSICIAN’S |
Indicate the telephone number where the physician can be contacted (preferably where records |
TELEPHONE NO: |
would be accessible pertaining to this patient) if more information is needed. |
QUESTION SECTION: |
This section is used to gather clinical information about the item or service billed. Answer each |
|
question which applies to the items ordered, checking “Y” for yes, “N” for no, a number if this is |
|
offered as an answer option, or fill in the blank if other information is requested. |
SUPPLIER |
The supplier’s signature certifies that the information on the form is an accurate representation |
ATTESTATION: |
of the situation(s) under which the item or service is billed. |
SUPPLIER |
After completion, supplier must sign and date the DME Information Form, |
SIGNATURE |
verifying the Attestation. |
AND DATE: |
|
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
DO NOT SUBMIT CLAIMS TO THIS ADDRESS. Please see http://www.medicare.gov/ for information on claim filing.
Form