

Handling PDF documents online is certainly a piece of cake with this PDF tool. You can fill out medicare complaint form pdf here effortlessly. To have our tool on the forefront of practicality, we aim to put into practice user-driven features and improvements on a regular basis. We're at all times happy to get feedback - join us in revampimg how you work with PDF forms. To get started on your journey, go through these basic steps:
Step 1: Just hit the "Get Form Button" at the top of this site to start up our pdf editor. This way, you'll find everything that is necessary to fill out your document.
Step 2: The tool allows you to customize your PDF file in various ways. Change it by writing customized text, correct what is originally in the document, and include a signature - all within the reach of a few clicks!
This form will involve specific information; to guarantee consistency, don't hesitate to pay attention to the guidelines hereunder:
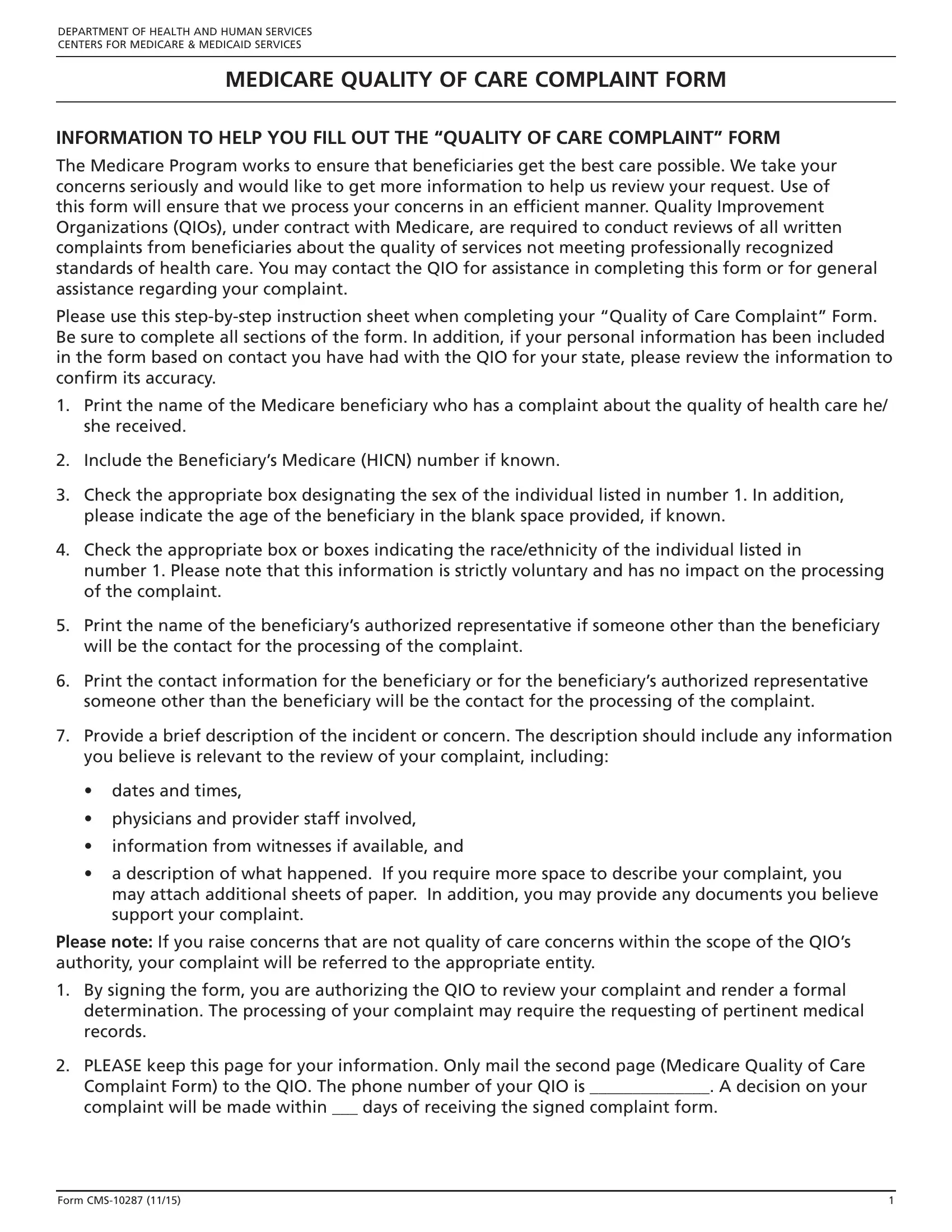
1. While submitting the medicare complaint form pdf, be sure to incorporate all essential blanks in the associated section. It will help to speed up the work, making it possible for your information to be processed promptly and correctly.

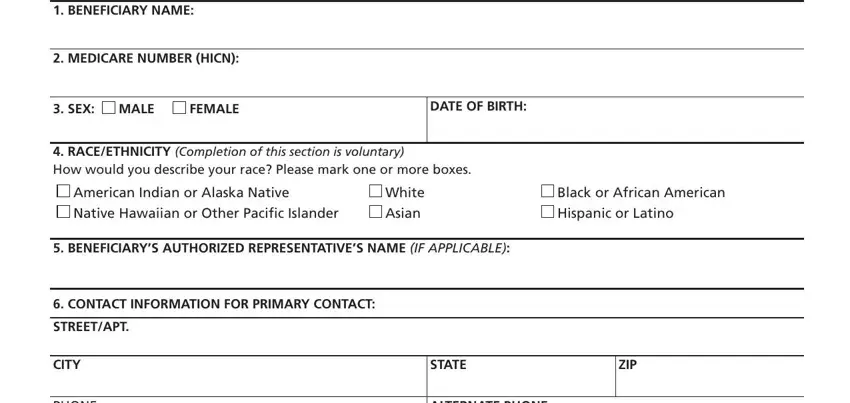
2. After performing this step, go on to the subsequent part and enter all required particulars in all these blank fields - BENEFICIARY NAME, MEDICARE NUMBER HICN, SEX MALE, FEMALE, DATE OF BIRTH, RACEETHNICITY Completion of this, American Indian or Alaska Native, Native Hawaiian or Other Pacific, White, Asian, Black or African American, Hispanic or Latino, BENEFICIARYS AUTHORIZED, CONTACT INFORMATION FOR PRIMARY, and STREETAPT.
3. This third segment should also be quite uncomplicated, PHONE, ALTERNATE PHONE, and Briefly Describe the incident or - each one of these form fields needs to be filled out here.
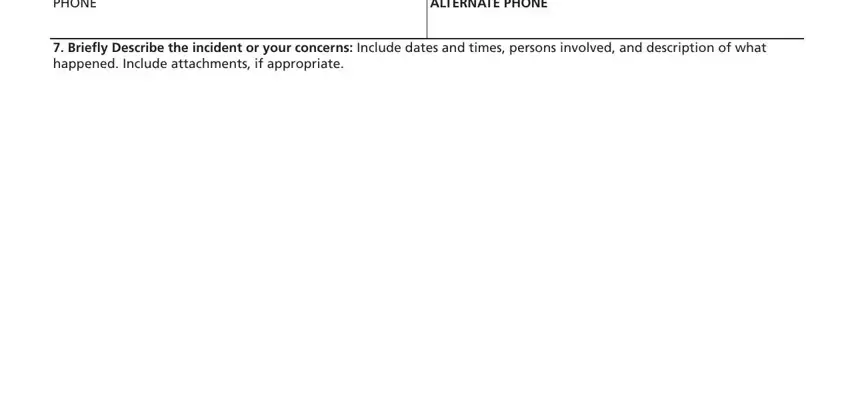
Always be really mindful when filling in Briefly Describe the incident or and ALTERNATE PHONE, as this is where most users make a few mistakes.
4. This fourth paragraph comes next with the next few blank fields to enter your details in: May we reveal your identity, YES, and Form CMS.

5. To wrap up your form, this last part requires a couple of extra fields. Filling out Check yes here if you authorize, YES, FOR YOUR INFORMATION If you have, By signing this form I am, SIGNATURE OF BENEFICIARY OR, DATE, and According to the Paperwork is going to finalize everything and you'll be done in the blink of an eye!
Step 3: Look through all the information you have entered into the form fields and click the "Done" button. Download the medicare complaint form pdf when you register at FormsPal for a 7-day free trial. Conveniently view the document within your FormsPal account, together with any modifications and adjustments being conveniently saved! With FormsPal, you're able to complete documents without the need to worry about personal information incidents or records getting shared. Our secure platform makes sure that your personal details are stored safe.