Department of Health and Human Services |
Form Approved OMB No.0938-0950 |
Centers for Medicare & Medicaid Services |
|
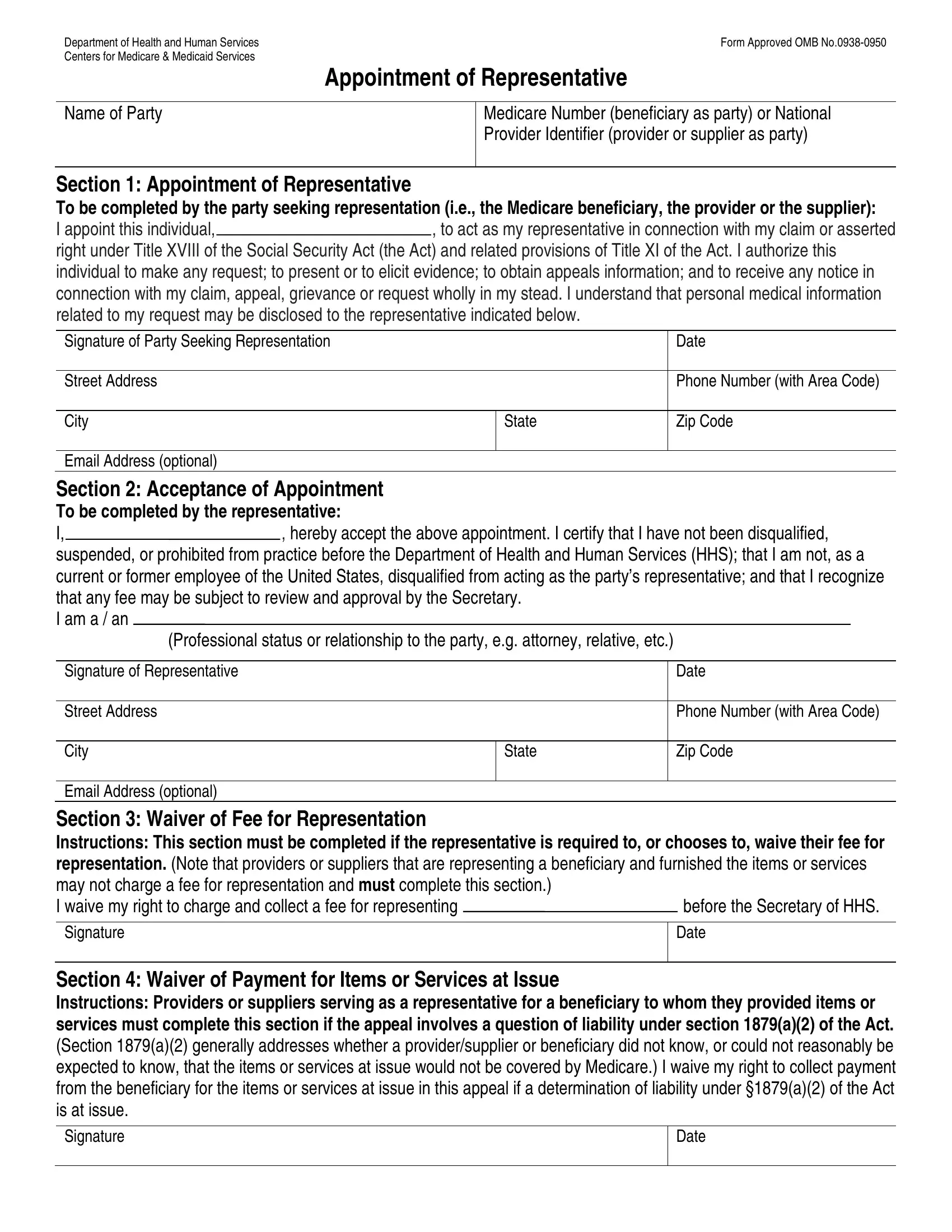
Appointment of Representative
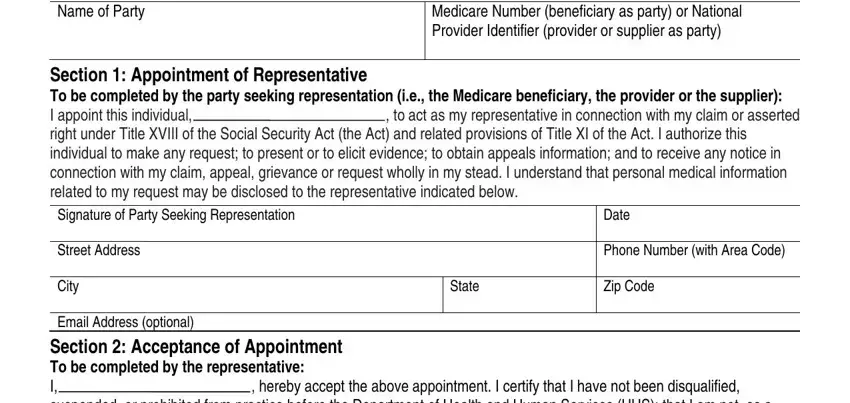
Medicare Number (beneficiary as party) or National Provider Identifier (provider or supplier as party)
Section 1: Appointment of Representative
To be completed by the party seeking representation (i.e., the Medicare beneficiary, the provider or the supplier):
I appoint this individual,, to act as my representative in connection with my claim or asserted right under Title XVIII of the Social Security Act (the Act) and related provisions of Title XI of the Act. I authorize this individual to make any request; to present or to elicit evidence; to obtain appeals information; and to receive any notice in connection with my claim, appeal, grievance or request wholly in my stead. I understand that personal medical information related to my request may be disclosed to the representative indicated below.
Signature of Party Seeking Representation |
|
Date |
|
|
|
Street Address |
|
Phone Number (with Area Code) |
|
|
|
City |
State |
Zip Code |
|
|
|
Email Address (optional) |
|
|
Section 2: Acceptance of Appointment
To be completed by the representative:
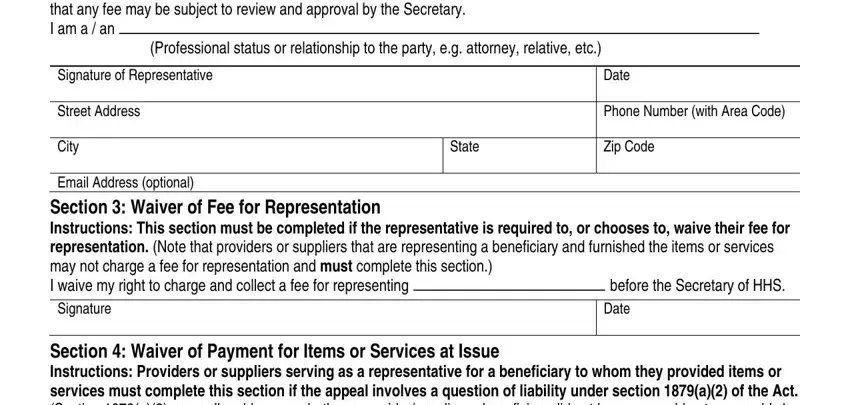
I,, hereby accept the above appointment. I certify that I have not been disqualified, suspended, or prohibited from practice before the Department of Health and Human Services (HHS); that I am not, as a current or former employee of the United States, disqualified from acting as the party’s representative; and that I recognize that any fee may be subject to review and approval by the Secretary.
I am a / an
(Professional status or relationship to the party, e.g. attorney, relative, etc.)
Signature of Representative |
|
Date |
|
|
|
Street Address |
|
Phone Number (with Area Code) |
|
|
|
City |
State |
Zip Code |
|
|
|
Email Address (optional)
Section 3: Waiver of Fee for Representation
Instructions: This section must be completed if the representative is required to, or chooses to, waive their fee for representation. (Note that providers or suppliers that are representing a beneficiary and furnished the items or services may not charge a fee for representation and must complete this section.)
I waive my right to charge and collect a fee for representing |
before the Secretary of HHS. |
Section 4: Waiver of Payment for Items or Services at Issue
Instructions: Providers or suppliers serving as a representative for a beneficiary to whom they provided items or services must complete this section if the appeal involves a question of liability under section 1879(a)(2) of the Act. (Section 1879(a)(2) generally addresses whether a provider/supplier or beneficiary did not know, or could not reasonably be expected to know, that the items or services at issue would not be covered by Medicare.) I waive my right to collect payment from the beneficiary for the items or services at issue in this appeal if a determination of liability under §1879(a)(2) of the Act is at issue.
Charging of Fees for Representing Beneficiaries before the Secretary of HHS
An attorney, or other representative for a beneficiary, who wishes to charge a fee for services rendered in connection with an appeal before the Secretary of HHS (i.e., an Administrative Law Judge (ALJ) hearing or attorney adjudicator review by the Office of Medicare Hearings and Appeals (OMHA), Medicare Appeals Council review, or a proceeding before OMHA or the Medicare Appeals Council as a result of a remand from federal district court) is required to obtain approval of the fee in accordance with 42 CFR 405.910(f).
The form, “Petition to Obtain Representative Fee” elicits the information required for a fee petition. It should be completed by the representative and filed with the request for ALJ hearing, OMHA review, or request for Medicare Appeals Council review. Approval of a representative’s fee is not required if: (1) the appellant being represented is a provider or supplier;
(2)the fee is for services rendered in an official capacity such as that of legal guardian, committee, or similar court appointed representative and the court has approved the fee in question; (3) the fee is for representation of a beneficiary in a proceeding in federal district court; or (4) the fee is for representation of a beneficiary in a redetermination or reconsideration. If the representative wishes to waive a fee, he or she may do so. Section III on the front of this form can be used for that purpose. In some instances, as indicated on the form, the fee must be waived for representation
Approval of Fee
The requirement for the approval of fees ensures that a representative will receive fair value for the services performed before HHS on behalf of a beneficiary, and provides the beneficiary with a measure of security that the fees are determined to be reasonable. In approving a requested fee, OMHA or Medicare Appeals Council will consider the nature and type of services rendered, the complexity of the case, the level of skill and competence required in rendition of the services, the amount of time spent on the case, the results achieved, the level of administrative review to which the representative carried the appeal and the amount of the fee requested by the representative.
Conflict of Interest
Sections 203, 205 and 207 of Title XVIII of the United States Code make it a criminal offense for certain officers, employees and former officers and employees of the United States to render certain services in matters affecting the Government or to aid or assist in the prosecution of claims against the United States. Individuals with a conflict of interest are excluded from being representatives of beneficiaries before HHS.
Where to Send This Form
Send this form to the same location where you are sending (or have already sent) your: appeal if you are filing an appeal, grievance or complaint if you are filing a grievance or complaint, or an initial determination or decision if you are requesting an initial determination or decision. If additional help is needed, contact 1-800-MEDICARE (1-800-633-4227) or your Medicare plan. TTY users please call 1-877-486-2048.
You have the right to get Medicare information in an accessible format, like large print, Braille, or audio. You also have the right to file a complaint if you believe you’ve been discriminated against. Visit https://www.cms.gov/about-cms/agency-
Information/aboutwebsite/cmsnondiscriminationnotice.html, or call 1-800-MEDICARE (1-800-633-4227) for more
information.
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0938-0950. The time required to prepare and distribute this collection is 15 minutes per notice, including the time to select the preprinted form, complete it and deliver it to the beneficiary. If you have comments concerning the accuracy of the time estimates or suggestions for improving this form, please write to CMS, PRA Clearance Officer, 7500 Security Boulevard, Baltimore, Maryland 21244-1850.
Form CMS-1696 (Rev 08/18)