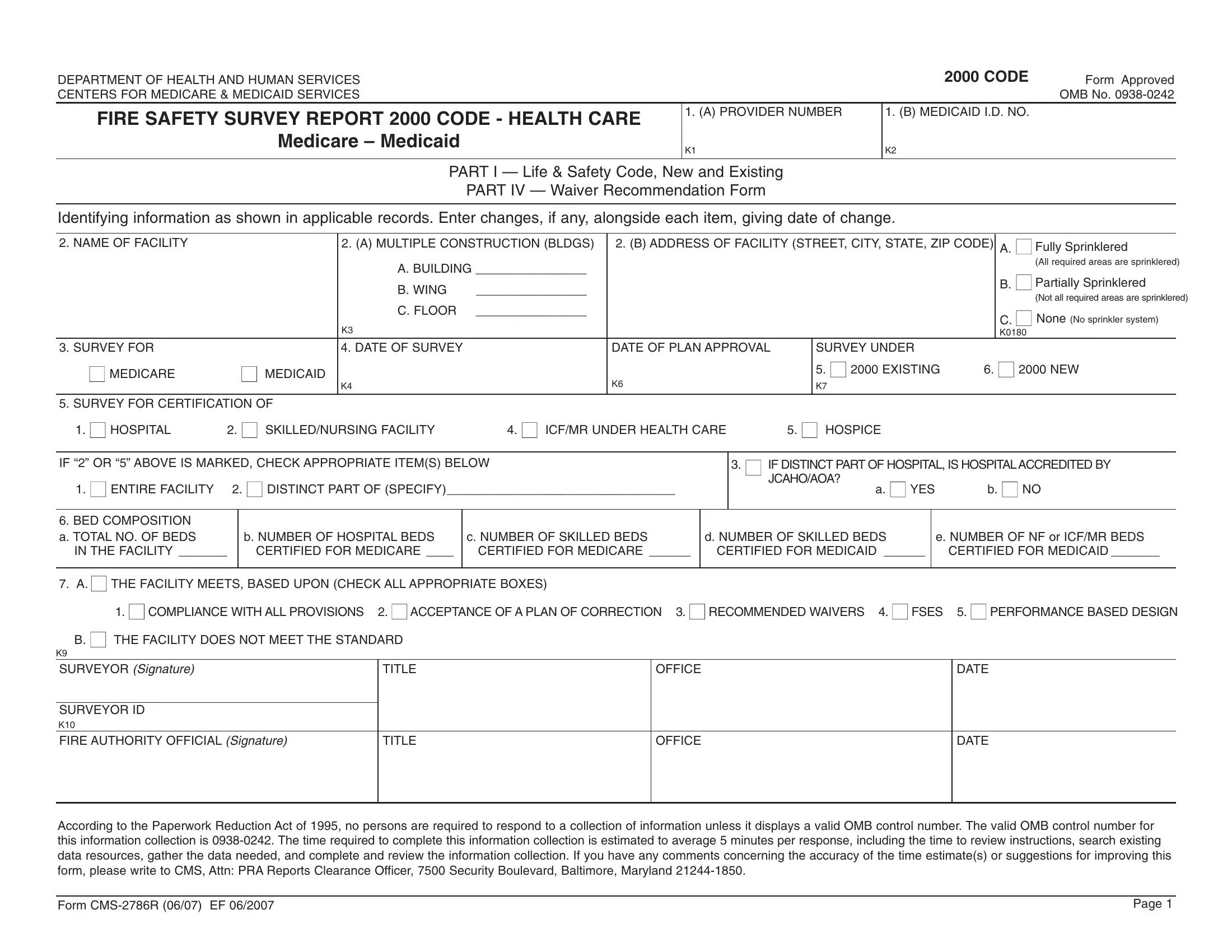
The CMS 2786R form, sanctioned by the Department of Health and Human Services and specifically the Centers for Medicare & Medicaid Services, is a critical component in ensuring fire safety within healthcare facilities, adhering to the 2000 Code. This document serves as a comprehensive fire safety survey report, guiding the evaluation of both new and existing buildings within the healthcare sector, from hospitals to skilled nursing facilities. Among its detailed items, the form addresses vital aspects such as the provider's information, building construction types, interior finishes, and the presence of sprinkler systems, specifying whether they are fully, partially, or not sprinklered. Moreover, it tackles the certification process for various healthcare services under Medicare and Medicaid, highlighting the importance of conforming to patient safety regulations through structural and fire safety standards. This form not only catalogues data regarding the facility's compliance with multiple safety provisions but also provides space for waiver recommendations and the implementation of plans of correction, ensuring that every healthcare facility meets or exceeds federal fire safety requirements. A unique feature of the form is its consideration of both the life safety code (Part I) and specific construction and design details, including but not limited to, the materials used in interior walls, fire resistance ratings, and the specifications of corridor walls and doors, ensuring a comprehensive approach to fire safety.
| Question | Answer |
|---|---|
| Form Name | Form Cms 2786R |
| Form Length | 27 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 6 min 45 sec |
| Other names | 2007, occupancies, fillable cms2786r form, ICF |
DEPARTMENT OF HEALTH AND HUMAN SERVICES |
|
2000 CODE |
Form Approved |
CENTERS FOR MEDICARE & MEDICAID SERVICES |
|
|
OMB No. |
FIRE SAFETY SURVEY REPORT 2000 CODE - HEALTH CARE |
1. (A) PROVIDER NUMBER |
1. (B) MEDICAID I.D. NO. |
|
|
|
|
|
Medicare – Medicaid |
K1 |
K2 |
|
|
|
||
|
|
|
|
PART I — Life & Safety Code, New and Existing
PART IV — Waiver Recommendation Form
Identifying information as shown in applicable records. Enter changes, if any, alongside each item, giving date of change.
2. NAME OF FACILITY |
|
2. (A) MULTIPLE CONSTRUCTION (BLDGS) |
2. (B) ADDRESS OF FACILITY (STREET, CITY, STATE, ZIP CODE) |
A. ■ Fully Sprinklered |
|
||||
|
|
A. BUILDING ________________ |
|
|
|
|
(All required areas are sprinklered) |
||
|
|
|
|
|
|
B. ■ Partially Sprinklered |
|||
|
|
B. WING |
________________ |
|
|
|
|
||
|
|
|
|
|
|
(Not all required areas are sprinklered) |
|||
|
|
|
|
|
|
|
|
||
|
|
C. FLOOR |
________________ |
|
|
|
|
C. ■ None (No sprinkler system) |
|
|
|
K3 |
|
|
|
|
|
||
|
|
|
|
|
|
|
K0180 |
||
|
|
|
|
|
|
|
|
||
3. SURVEY FOR |
|
4. DATE OF SURVEY |
|
DATE OF PLAN APPROVAL |
|
SURVEY UNDER |
|
|
|
■ MEDICARE |
■ MEDICAID |
|
|
|
|
5. ■ 2000 EXISTING |
6. ■ 2000 NEW |
||
|
|
K6 |
|
|
|
|
|
||
|
|
K4 |
|
|
K7 |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
5. SURVEY FOR CERTIFICATION OF |
|
|
|
|
|
|
|
||
1. ■ HOSPITAL |
2. ■ SKILLED/NURSING FACILITY |
4. ■ ICF/MR UNDER HEALTH CARE |
5. ■ HOSPICE |
|
|
|
|||
IF “2” OR “5” ABOVE IS MARKED, CHECK APPROPRIATE ITEM(S) BELOW
1. ■ ENTIRE FACILITY 2. ■ DISTINCT PART OF (SPECIFY)_________________________________
3. ■ IF DISTINCT PART OF HOSPITAL, IS HOSPITALACCREDITED BY |
|
JCAHO/AOA? |
|
a. ■ YES |
b. ■ NO |
6. BED COMPOSITION a. TOTAL NO. OF BEDS
IN THE FACILITY _______
b. NUMBER OF HOSPITAL BEDS CERTIFIED FOR MEDICARE ____
c. NUMBER OF SKILLED BEDS CERTIFIED FOR MEDICARE ______
d. NUMBER OF SKILLED BEDS CERTIFIED FOR MEDICAID ______
e. NUMBER OF NF or ICF/MR BEDS CERTIFIED FOR MEDICAID _______
7. A. ■ THE FACILITY MEETS, BASED UPON (CHECK ALL APPROPRIATE BOXES) |
|
|
|
|
|
1. ■ COMPLIANCE WITH ALL PROVISIONS |
2. ■ ACCEPTANCE OF A PLAN OF CORRECTION 3. ■ RECOMMENDED WAIVERS |
4. ■ FSES 5. ■ PERFORMANCE BASED DESIGN |
|||
B. ■ THE FACILITY DOES NOT MEET THE STANDARD |
|
|
|
|
|
K9 |
|
|
|
|
|
SURVEYOR (Signature) |
TITLE |
OFFICE |
|
DATE |
|
|
|
|
|
|
|
SURVEYOR ID |
|
|
|
|
|
K10 |
|
|
|
|
|
FIRE AUTHORITY OFFICIAL (Signature) |
TITLE |
OFFICE |
|
DATE |
|
|
|
|
|
|
|
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
Form |
Page 1 |
|
Name of Facility |
|
|
|
|
2000 CODE |
|||
|
|
|
|
|
|
|
|
|
|
|
ID |
|
|
|
MET |
NOT |
N/A |
REMARKS |
|
|
PREFIX |
|
|
|
MET |
||||
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
PART I - LSC REQUIREMENTS - Items in italics relate to the FSES |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BUILDING CONSTRUCTION |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
K11 If the building has a common wall with a nonconforming building, |
|
|
|
|||||
|
|
the common wall is a fire barrier having at least a two hour fire |
|
|
|
||||
|
|
resistance rating constructed of materials as required for the |
|
|
|
||||
|
|
addition. Communicating openings occur only in corridors and |
|
|
|
||||
|
|
shall be protected by approved |
|
|
|
||||
|
18.1.1.4.1, 18.1.1.4.2, 19.1.1.4.1, 19.1.1.4.2 |
|
|
|
|
||||
|
|
|
|
|
|
|
|||
|
K12 2000 EXISTING |
|
|
|
|
|
|||
|
|
Building construction type and height meets one of the following: |
|
|
|
||||
|
19.1.6.2, 19.1.6.3, 19.1.6.4, 19.3.5.1 |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
1 |
|
I (443), I (332), II (222) |
Any Height |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
II (111) |
One story only |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not over three stories with |
|
|
|
|
|
3 |
|
II (111) |
complete automatic |
|
|
|
|
|
|
|
|
|
|
sprinkler system. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
III (211) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
V (111) |
Not over two stories with |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
complete automatic |
|
|
|
|
|
6 |
|
IV (2HH) |
|
|
|
|
||
|
|
sprinkler system. |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
7 |
|
II (000) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
III (200) |
Not over one story with |
|
|
|
|
|
|
|
|
|
|
complete automatic |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
V (000) |
sprinkler system. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
■Building contains fire treated wood.
Give a brief description, in REMARKS, of the construction, the number of stories, including basements, floors on which patients are located, location of smoke or fire barriers and dates of approval. Complete sketch or attach small floor plan of the building as appropriate.
Form |
Page 2 |
Name of Facility |
|
|
|
|
2000 CODE |
|||
|
|
|
|
|
|
|
|
|
ID |
|
|
|
MET |
NOT |
N/A |
REMARKS |
|
PREFIX |
|
|
|
MET |
||||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
K12 2000 NEW |
|
|
|
|
|
|||
|
Building construction type and height meets one of the following: |
|
|
|
||||
18.1.6.2, 18.1.6.3, 18.2.5.1 |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
1 |
|
I (443), I (332), II (222) |
Any height with complete |
|
|
|
|
|
|
automatic sprinkler system |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not over three stories |
|
|
|
|
2 |
|
II (111) |
with complete automatic |
|
|
|
|
|
|
|
|
|
sprinkler system |
|
|
|
|
|
3 |
|
III (211) |
|
|
|
|
|
|
|
|
|
Not over one story with |
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
V (111) |
complete automatic |
|
|
|
|
|
|
|
|
|
sprinkler system. |
|
|
|
|
5 |
|
IV (2HH) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
II (000) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
III (200) |
|
|
|
|
|
|
|
|
|
|
Not Permitted |
|
|
|
|
8 |
|
V (000) |
|
|
|
|
||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
■Building contains fire treated wood.
Give a brief description, in REMARKS, of the construction, the number of stories, including basements, floors on which patients are located, location of smoke or fire barriers and dates of approval. Complete sketch or attach small floor plan of the building as appropriate.
K103 Interior walls and partitions in buildings of Type I or Type II construction shall be noncombustible or
(Indicate N/A for existing buildings using listed fire retardant treated wood studs within
Form |
Page 3 |
Name of Facility |
|
|
|
|
2000 CODE |
|
|
|
|
|
|
ID |
|
MET |
NOT |
N/A |
REMARKS |
PREFIX |
|
MET |
|||
|
|
|
|
||
|
|
|
|
|
|
|
INTERIOR FINISH |
|
|
|
|
|
|
|
|
|
|
K14 2000 EXISTING |
|
|
|
|
|
|
Interior finish for corridors and exitways, including exposed |
|
interior surfaces of buildings such as fixed or movable walls, |
|
partitions, columns, and ceilings has a flame spread rating of |
|
Class A or Class B. 19.3.3.1, 19.3.3.2 |
|
Indicate flame spread rating/s _________ |
|
2000 NEW |
|
Interior finish for corridors and exitways, including exposed |
|
interior surfaces of buildings such as fixed or movable walls, |
|
partitions, columns, and ceilings has a flame spread rating of |
|
Class A or Class B. Lower portion of corridor walls can be |
|
Class C. 18.3.3.1, 18.3.3.2 |
|
Indicate flame spread rating/s_________ |
|
|
K15 |
2000 EXISTING |
|
Interior finish for rooms and spaces not used for corridors or |
|
exitways, including exposed interior surfaces of buildings such |
|
as fixed or movable walls, partitions, columns, and ceilings has |
|
a flame spread rating of Class A or Class B. (In |
|
buildings, flame spread rating of Class A, Class B, or Class C |
|
may be continued in use within rooms separated in accordance |
|
with 19.3.6 from the access corridors.) 19.3.3.1, 19.3.3.2 |
|
Indicate flame spread rating/s_________ |
|
2000 NEW |
|
Interior finish for rooms and spaces not used for corridors or |
|
exitways, including exposed interior surfaces of buildings such |
|
as fixed or movable walls, partitions, columns, and ceilings has |
|
a flame spread rating of Class A or Class B. (Rooms not over |
|
4 persons in capacity may have a flame spread rating of Class A, |
|
Class B, or Class C). 18.3.3.1, 18.3.3.2. |
|
Indicate flame spread rating/s_________ |
Form |
Page 4 |

Name of Facility |
|
|
2000 CODE |
||
|
|
|
|
|
|
ID |
|
MET |
NOT |
N/A |
REMARKS |
PREFIX |
|
MET |
|||
|
|
|
|
||
|
|
|
|
|
|
K16 |
Newly installed interior floor finish complying with 10.2.7 shall be |
|
|
|
|
|
permitted in corridors and exits if Class I. 18.3.3.3, 19.3.3.3 |
|
|
|
|
|
(Indicate N/A for existing interior floor finish.) |
|
|
|
|
|
In smoke compartments protected throughout by an approved, |
|
|
|
|
|
supervised automatic sprinkler system in accordance with |
|
|
|
|
|
19.3.5.2, no interior floor finish requirements shall apply. |
|
|
|
|
|
|
|
|
|
|
|
CORRIDOR WALLS AND DOORS |
|
|
|
|
|
|
|
|
|
|
K17 |
2000 EXISTING |
|
|
|
|
|
Corridors are separated from use areas by walls constructed with |
|
|
|
|
|
at least 1/2 hour fire resistance rating. In fully sprinklered smoke |
|
|
|
|
|
compartments, partitions are only required to resist the passage |
|
|
|
|
|
of smoke. In |
|
|
|
|
|
above the ceiling. (Corridor walls may terminate at the underside |
|
|
|
|
|
of ceilings where specifically permitted by Code. Charting and |
|
|
|
|
|
clerical stations, waiting areas, dining rooms, and activity spaces |
|
|
|
|
|
may be open to corridor under certain conditions specified in the |
|
|
|
|
|
Code. Gift shops may be separated from corridors by |
|
|
|
|
|
rated walls if the gift shop is fully sprinklered.) |
|
|
|
|
|
19.3.6.1, 19.3.6.2.1, 19.3.6.5 |
|
|
|
|
|
If the walls have a fire resistance rating, give rating_________ |
|
|
|
|
|
if the walls terminate at the underside of a ceiling, give a brief |
|
|
|
|
|
description in REMARKS, of the ceiling, describing the ceiling |
|
|
|
|
|
throughout the floor area. |
|
|
|
|
|
2000 NEW |
|
|
|
|
|
Corridor walls shall form a barrier to limit the transfer of smoke. |
|
|
|
|
|
Such walls shall be permitted to terminate at the ceiling where |
|
|
|
|
|
the ceiling is constructed to limit the transfer of smoke. No fire |
|
|
|
|
|
resistance rating is required for the corridor walls. |
|
|
|
|
|
18.3.6.1, 18.3.6.2, 18.3.6.5 |
|
|
|
|
|
|
|
|
|
|
Form |
Page 5 |