
Once you open the online PDF editor by FormsPal, you're able to complete or change certification esrd right here and now. Our team is focused on providing you with the perfect experience with our editor by consistently presenting new functions and improvements. With these updates, using our tool becomes better than ever before! With just a few basic steps, you are able to start your PDF editing:
Step 1: First of all, access the editor by pressing the "Get Form Button" above on this site.
Step 2: After you open the online editor, there'll be the document prepared to be filled out. Apart from filling in different blanks, you might also do some other things with the PDF, such as adding any text, modifying the original textual content, adding graphics, putting your signature on the document, and more.
For you to fill out this document, make sure that you type in the necessary information in each blank:
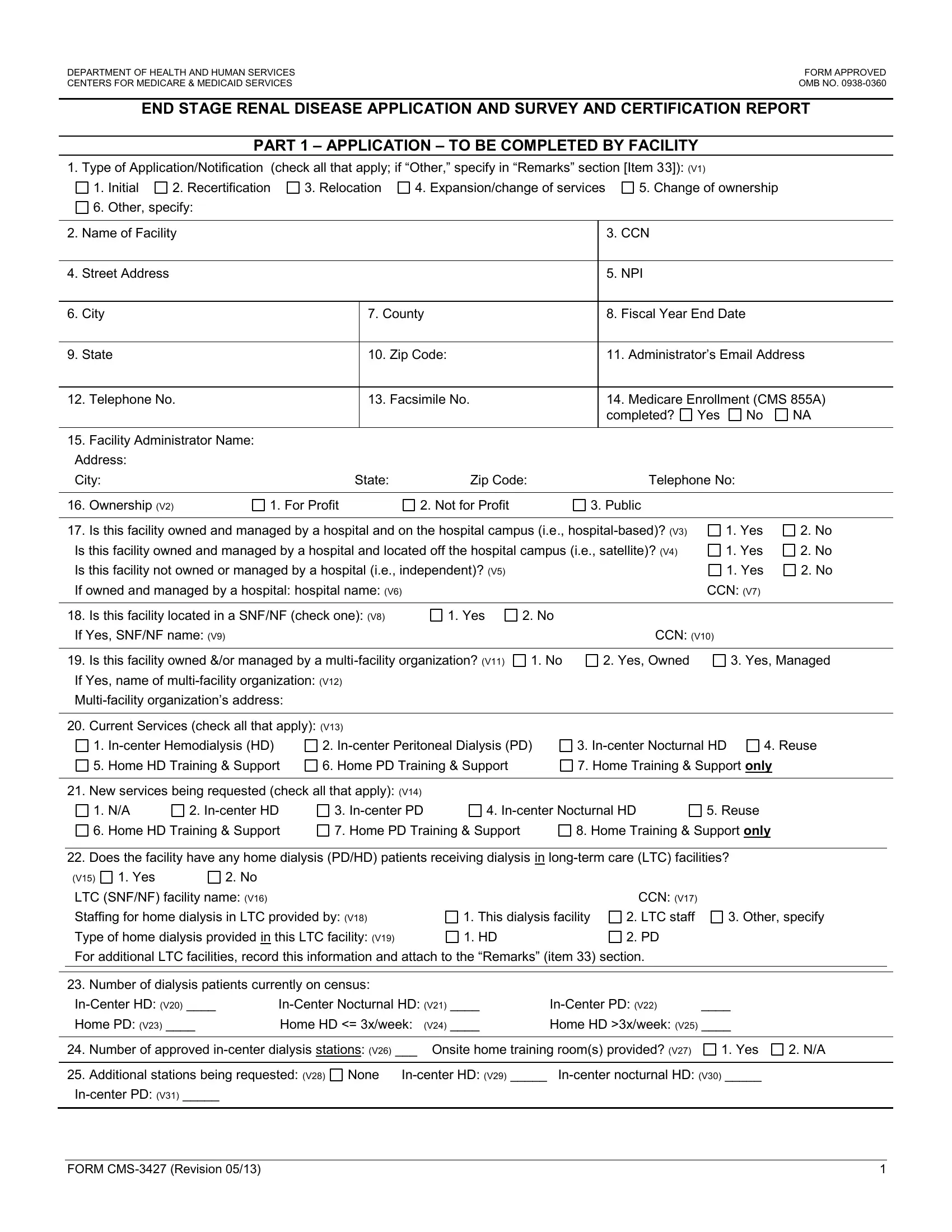
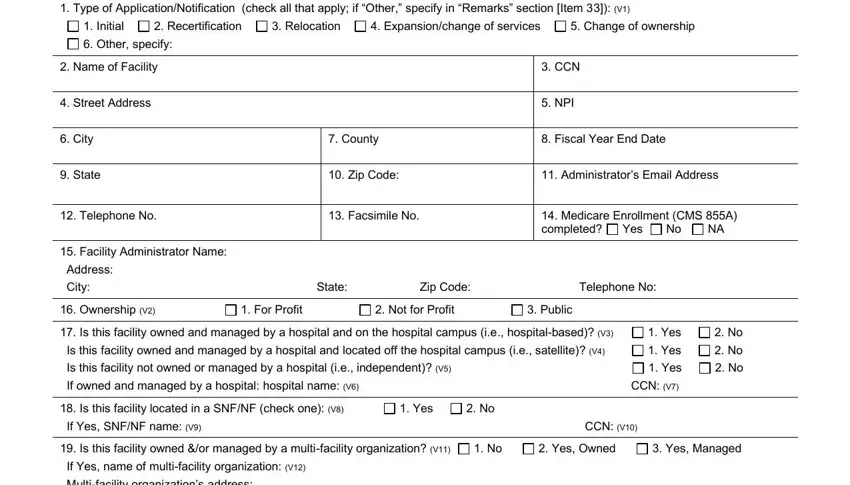
1. The certification esrd will require specific details to be entered. Ensure the subsequent blanks are completed:
2. Once the last part is completed, you're ready include the required specifics in Current Services check all that, Incenter Hemodialysis HD, Incenter Peritoneal Dialysis PD, Incenter Nocturnal HD, Reuse, Home HD Training Support, Home PD Training Support, Home Training Support only, New services being requested, Incenter HD, Incenter PD, Incenter Nocturnal HD, Reuse, Home HD Training Support, and Home PD Training Support so you're able to move on further.
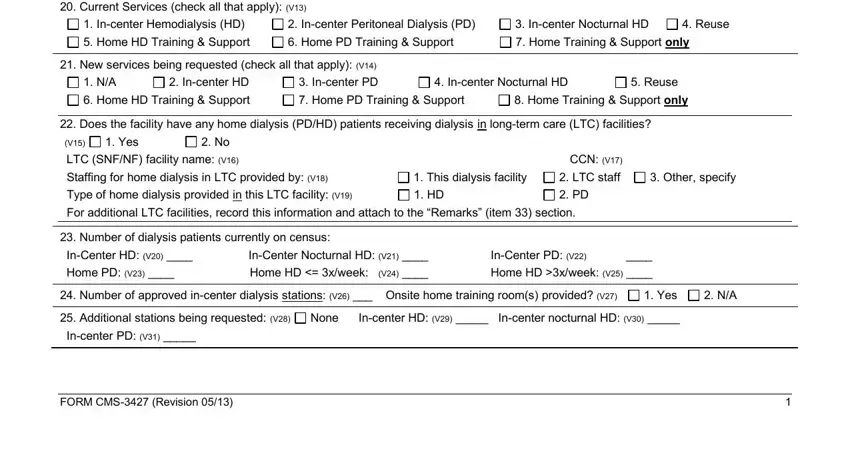
Be really attentive while completing Home PD Training Support and Reuse, because this is the part where many people make errors.
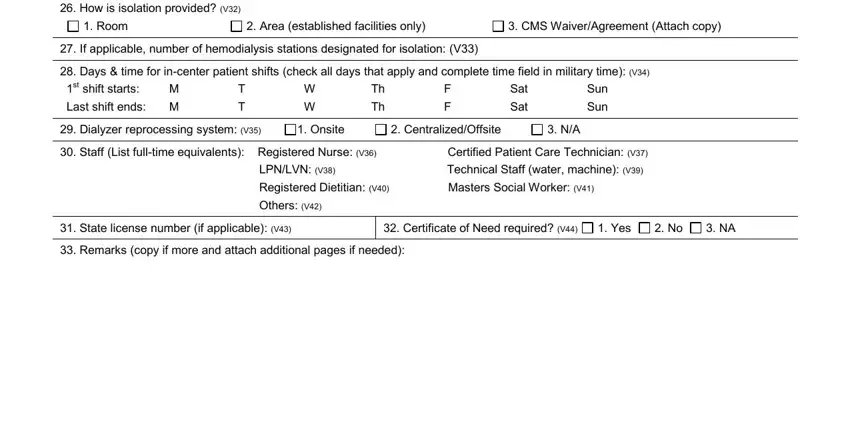
3. Throughout this step, examine How is isolation provided V, Room, Area established facilities only, CMS WaiverAgreement Attach copy, If applicable number of, Days time for incenter patient, Dialyzer reprocessing system V, Onsite, CentralizedOffsite, Staff List fulltime equivalents, LPNLVN V Technical Staff water, Registered Dietitian V Masters, Others V, State license number if, and Yes. These have to be filled in with greatest attention to detail.
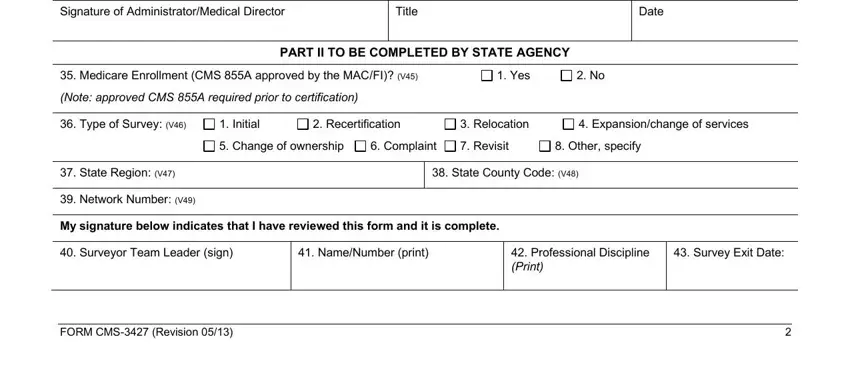
4. Completing Signature of AdministratorMedical, Title, Date, Medicare Enrollment CMS A, Yes, Note approved CMS A required prior, PART II TO BE COMPLETED BY STATE, Type of Survey V, Initial, Recertification, Relocation, Expansionchange of services, Change of ownership, Complaint, and Revisit is crucial in this part - ensure that you be patient and fill in each and every blank!
Step 3: Once you have looked over the details provided, click on "Done" to conclude your FormsPal process. Right after creating a7-day free trial account here, you'll be able to download certification esrd or email it without delay. The file will also be readily accessible from your personal account page with all your edits. FormsPal guarantees your data privacy by using a secure system that never records or distributes any type of private information used in the file. You can relax knowing your docs are kept confidential every time you use our editor!