

Once you open the online PDF editor by FormsPal, you are able to complete or change hospice request certification medicare here and now. FormsPal is aimed at providing you the absolute best experience with our editor by consistently presenting new functions and enhancements. Our tool has become much more useful as the result of the newest updates! Now, filling out PDF forms is easier and faster than ever before. Getting underway is easy! All you need to do is follow the following simple steps below:
Step 1: First of all, open the pdf editor by clicking the "Get Form Button" at the top of this page.
Step 2: This tool gives you the capability to modify your PDF form in a range of ways. Change it with customized text, correct what's already in the document, and put in a signature - all within the reach of several clicks!
When it comes to fields of this specific document, here's what you want to do:
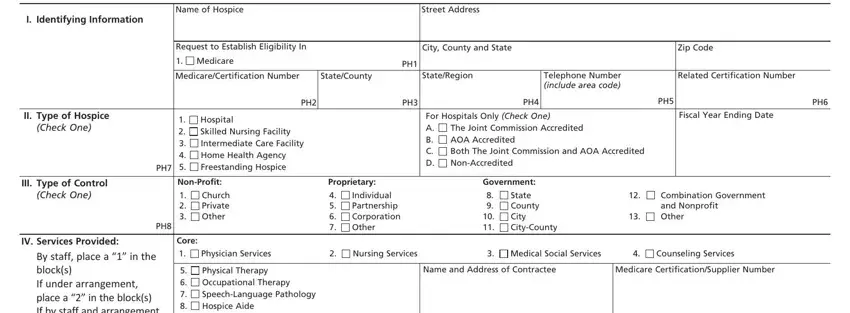
1. It's essential to fill out the hospice request certification medicare accurately, hence take care while filling out the areas that contain all these fields:
2. Once the previous segment is done, you'll want to include the needed details in By staff place a in the blocks If, Physical Therapy Occupational, Medical Supplies, Short Term lnpatient Care, PHO, A Acute B Respite, V Number of Employees, Volunteers Fulltime Equivalent Top, Physicians, Registered Professional Nurses PH, Employees, Volunteers, Employees, Volunteers, and Licensed Practical Nurses Licensed so that you can go further.
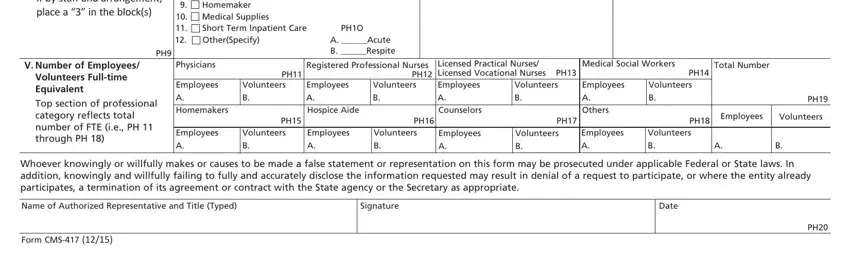
Always be really attentive while filling in Registered Professional Nurses PH and Physicians, as this is where a lot of people make errors.
Step 3: Immediately after taking another look at your completed blanks, press "Done" and you're all set! After setting up afree trial account here, it will be possible to download hospice request certification medicare or send it through email right away. The form will also be readily available in your personal account menu with all your edits. With FormsPal, you can easily complete documents without needing to be concerned about personal data incidents or entries being shared. Our protected system ensures that your private information is stored safely.