

You'll be able to work with cms 588 easily with our PDFinity® online tool. In order to make our editor better and more convenient to work with, we consistently implement new features, taking into account feedback coming from our users. Here's what you would need to do to get started:
Step 1: First, access the editor by pressing the "Get Form Button" in the top section of this page.
Step 2: Once you start the PDF editor, you'll notice the form ready to be filled in. In addition to filling out different blanks, you may as well do some other actions with the form, that is putting on any textual content, changing the initial text, adding illustrations or photos, signing the form, and much more.
For you to finalize this PDF document, make sure that you provide the required information in every area:
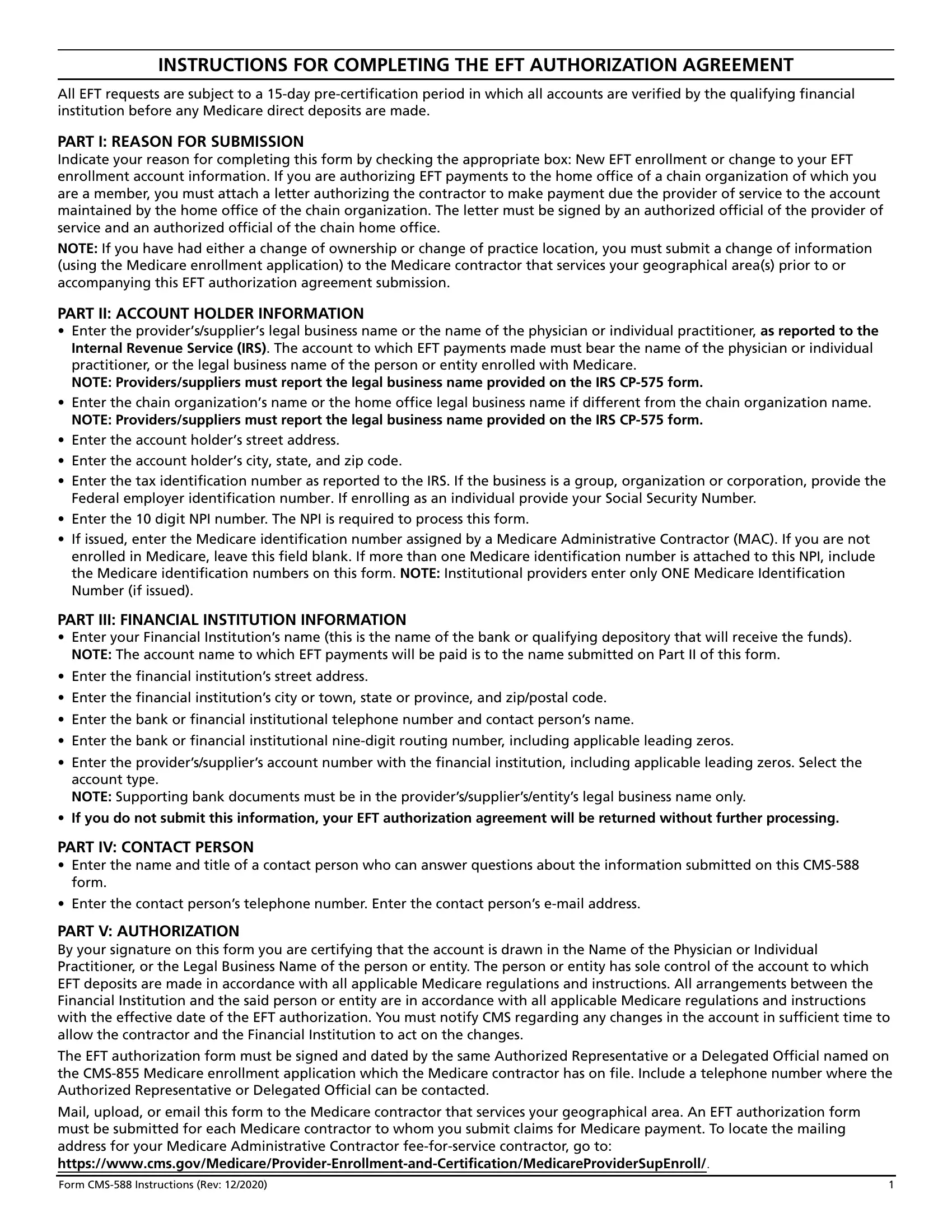
1. When submitting the cms 588, make sure to include all of the needed fields in its corresponding section. It will help expedite the work, allowing for your information to be processed quickly and appropriately.
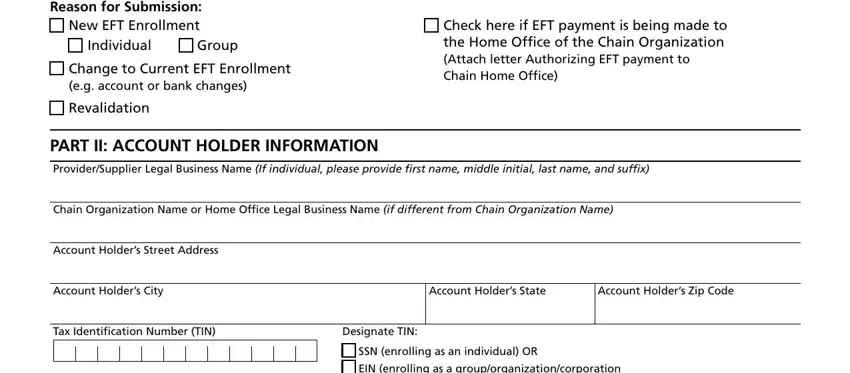
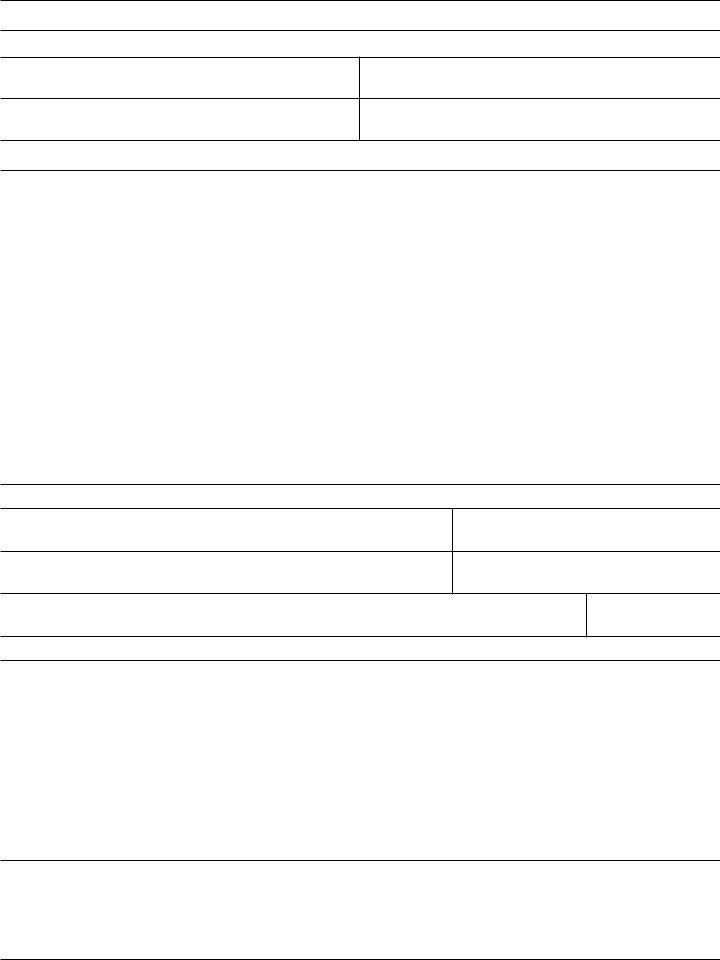
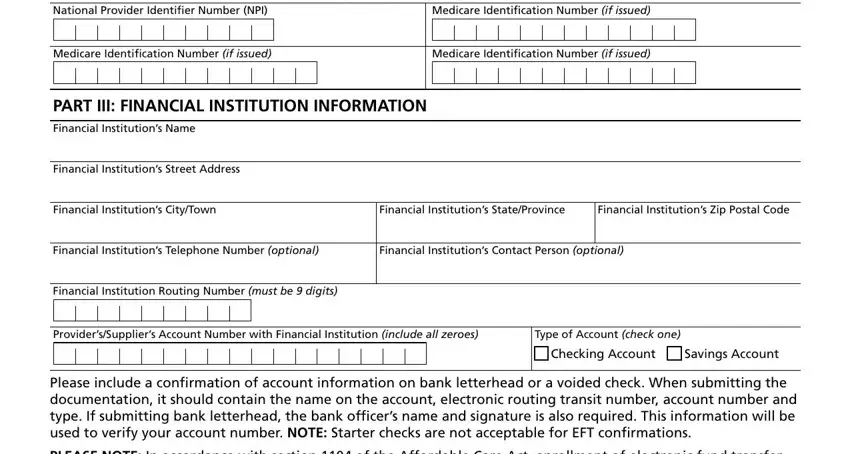
2. Once your current task is complete, take the next step – fill out all of these fields - National Provider Identifier, Medicare Identification Number if, SSN enrolling as an individual OR, Medicare Identification Number if, Medicare Identification Number if, PART III FINANCIAL INSTITUTION, Financial Institutions Name, Financial Institutions Street, Financial Institutions CityTown, Financial Institutions, Financial Institutions Zip Postal, Financial Institutions Telephone, Financial Institutions Contact, Financial Institution Routing, and ProvidersSuppliers Account Number with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
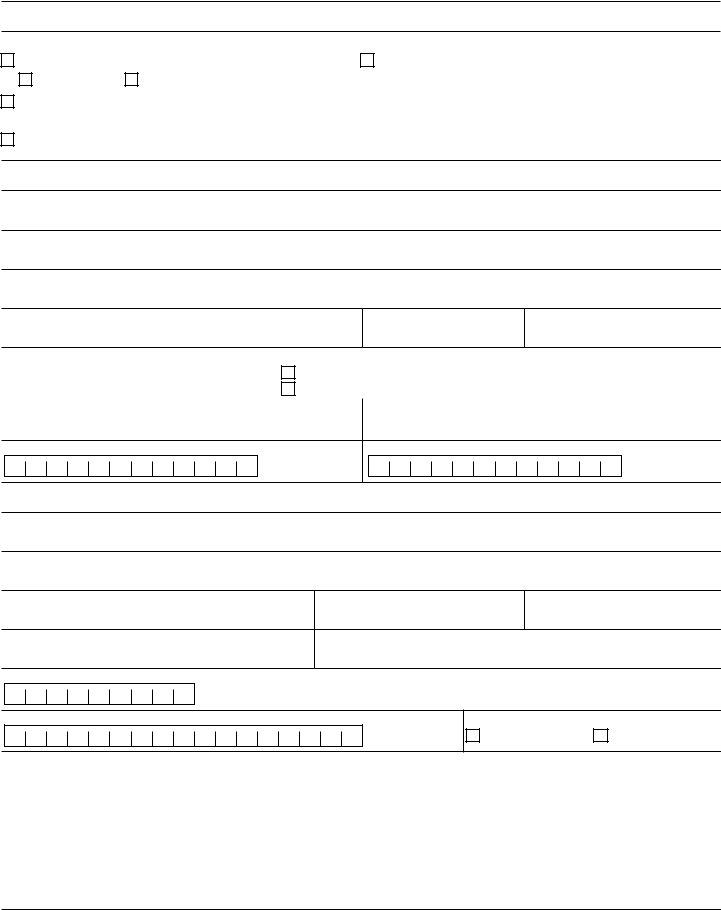
3. The following step should also be pretty straightforward, Contact Persons Name, Contact Persons Title, Contact Persons Telephone Number, Contact Persons Email Address, PART V AUTHORIZATION, I hereby authorize the Centers for, If payment is being made to an, If the account is drawn in the, and This authorization agreement is - these form fields will have to be filled in here.
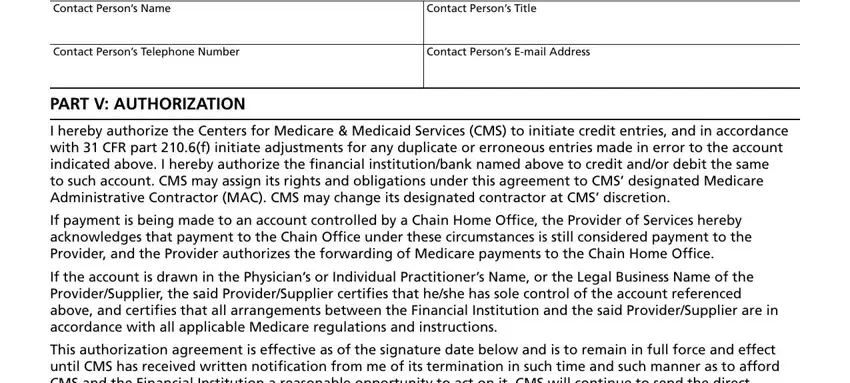
Concerning Contact Persons Email Address and This authorization agreement is, make sure that you take another look in this section. These two are surely the most important ones in this file.
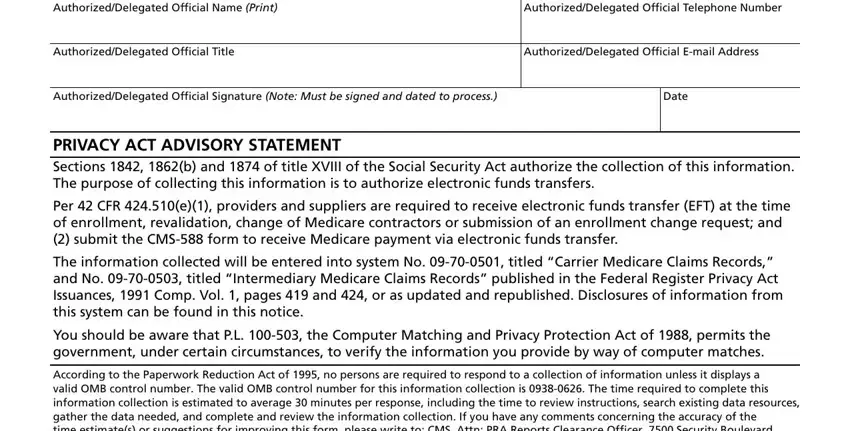
4. The next subsection will require your information in the following parts: SIGNATURE LINE AuthorizedDelegated, AuthorizedDelegated Official, AuthorizedDelegated Official Title, AuthorizedDelegated Official Email, AuthorizedDelegated Official, Date, PRIVACY ACT ADVISORY STATEMENT, Per CFR e providers and suppliers, The information collected will be, You should be aware that PL the, and According to the Paperwork. Make sure that you fill out all requested information to go onward.
Step 3: After double-checking your fields, press "Done" and you are good to go! Make a 7-day free trial account at FormsPal and obtain direct access to cms 588 - which you'll be able to then use as you would like inside your FormsPal account page. When you work with FormsPal, you're able to complete documents without the need to get worried about database breaches or records getting shared. Our protected system ensures that your personal data is stored safely.