




Using PDF forms online can be simple with our PDF editor. Anyone can fill in Form Cms R 0235St here and use various other functions we offer. To retain our tool on the leading edge of convenience, we work to integrate user-oriented features and improvements regularly. We're routinely thankful for any suggestions - assist us with remolding how you work with PDF documents. Starting is simple! All you need to do is take the next basic steps down below:
Step 1: Click on the "Get Form" button above on this page to get into our editor.
Step 2: This editor helps you work with the majority of PDF documents in many different ways. Change it with personalized text, correct what's already in the PDF, and put in a signature - all within a few mouse clicks!
This form will require particular information to be typed in, thus you should definitely take whatever time to type in exactly what is asked:
1. Fill out your Form Cms R 0235St with a number of major fields. Note all of the required information and ensure absolutely nothing is neglected!
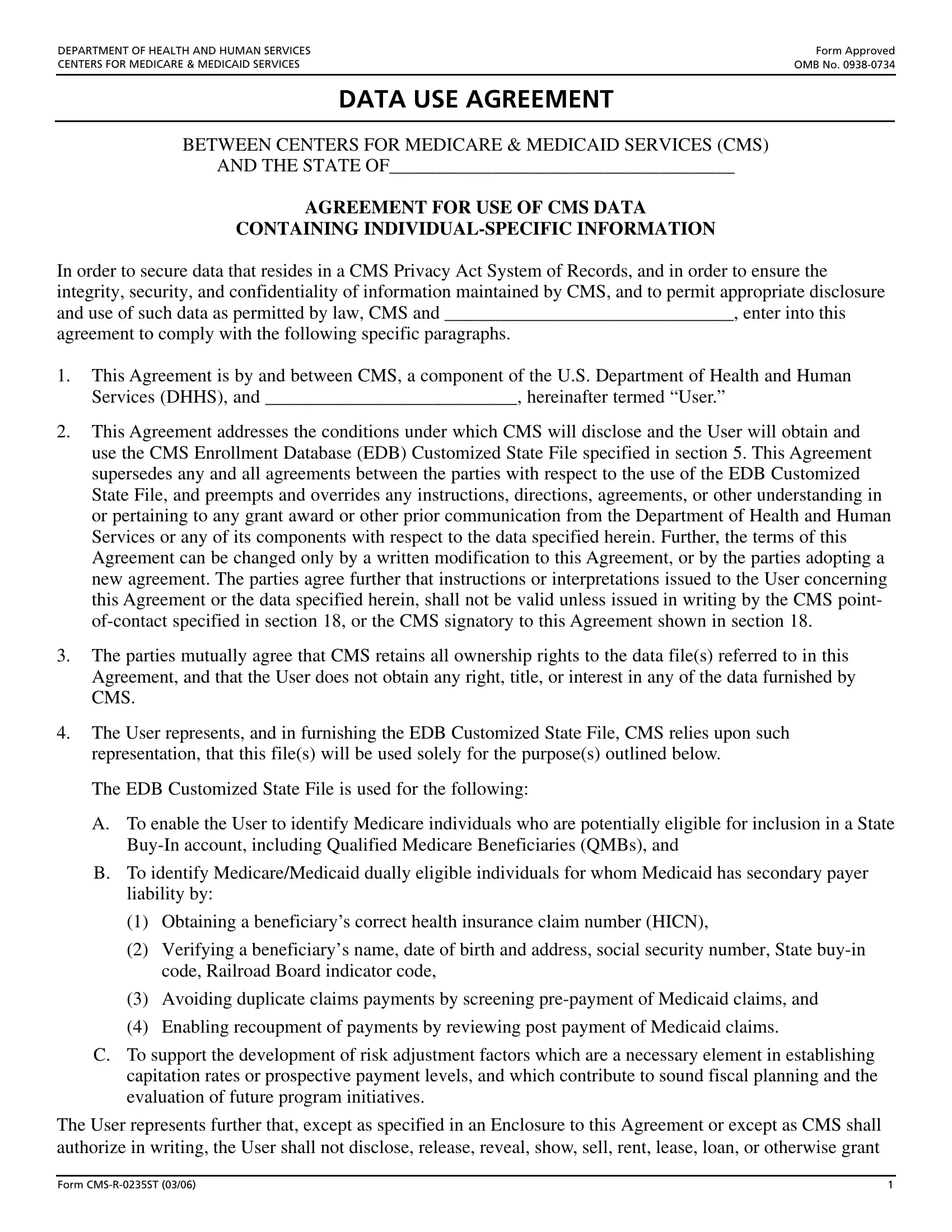
2. Once your current task is complete, take the next step – fill out all of these fields - File, EDB Customized State File, Years, Current, The parties mutually agree that, and The User agrees to establish with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. In this part, review The parties mutually agree that, The User agrees that in the event, or may have made disclosure of the, The User hereby acknowledges that, and a including a fine not exceeding. These have to be filled out with highest accuracy.
4. The fourth paragraph comes next with all of the following form blanks to fill out: NameTitle of User typed or printed, State AgencyOrganization, Street Address, City, State, ZIP Code, Phone Number including area code, Email Address if applicable, Signature, Date, and The parties mutually agree that.
5. To wrap up your document, this last section includes a number of extra blanks. Completing Name of Custodian typed or printed, CompanyOrganization, Street Address, City, State, ZIP Code, Phone Number including area code, Email Address if applicable, Signature, Date, and Form CMSRST is going to conclude everything and you're going to be done very fast!
A lot of people often make mistakes when filling in Form CMSRST in this part. You should definitely read again whatever you type in right here.
Step 3: Prior to moving on, double-check that form fields have been filled out the proper way. Once you establish that it's correct, click on “Done." After registering afree trial account at FormsPal, you will be able to download Form Cms R 0235St or send it via email directly. The PDF document will also be easily accessible from your personal account with all your adjustments. FormsPal is committed to the privacy of our users; we always make sure that all information put into our editor is kept secure.