
When you need to fill out Form Csf 01 0100, you don't have to download any software - just try using our online PDF editor. FormsPal team is dedicated to giving you the best possible experience with our editor by constantly introducing new functions and upgrades. With all of these improvements, using our editor gets easier than ever before! By taking a few easy steps, you can begin your PDF journey:
Step 1: Press the "Get Form" button above on this page to access our tool.
Step 2: The editor enables you to work with PDF files in many different ways. Enhance it with customized text, correct existing content, and place in a signature - all manageable in no time!
This form requires some specific details; in order to guarantee consistency, make sure you take heed of the subsequent guidelines:
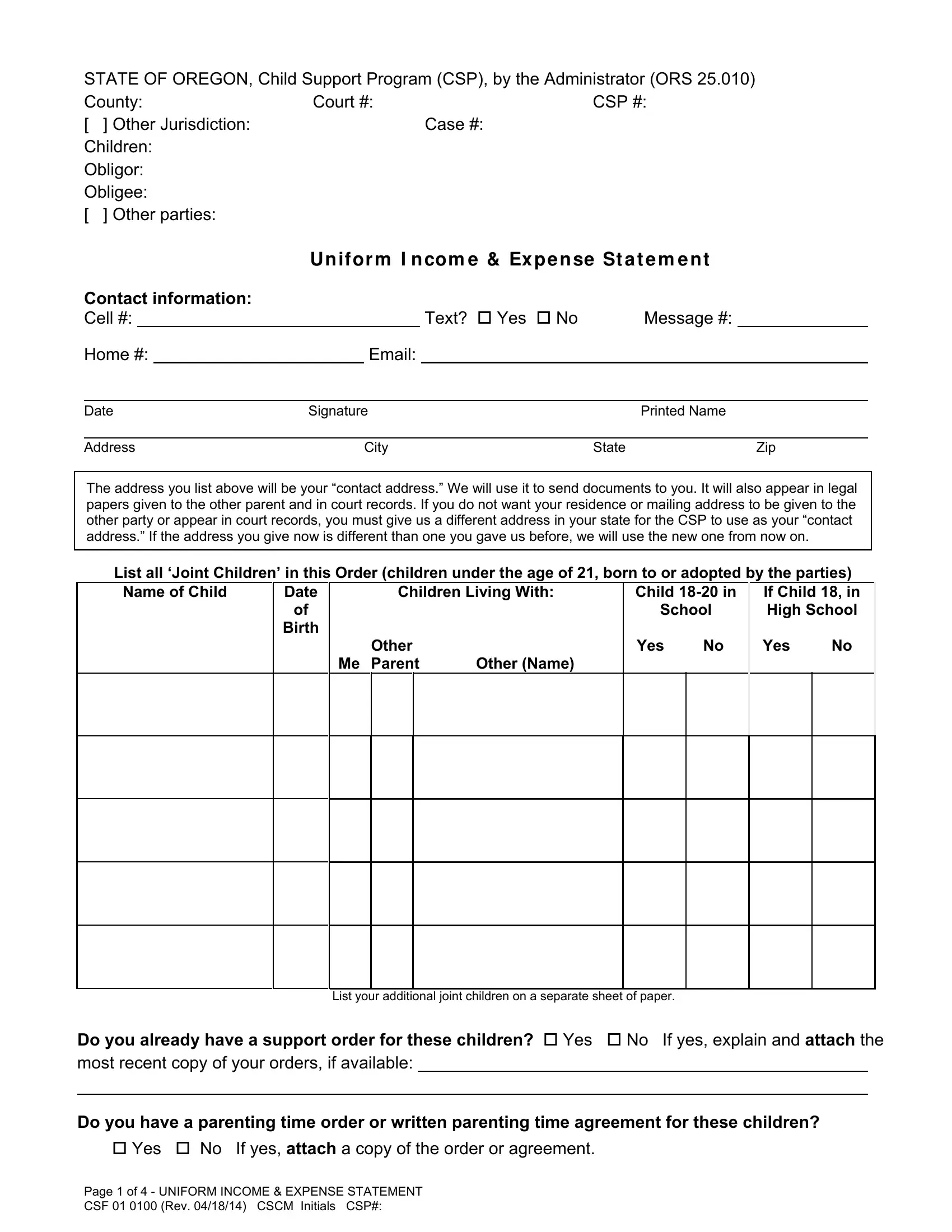
1. You have to fill out the Form Csf 01 0100 accurately, so be careful while working with the areas containing all of these blank fields:
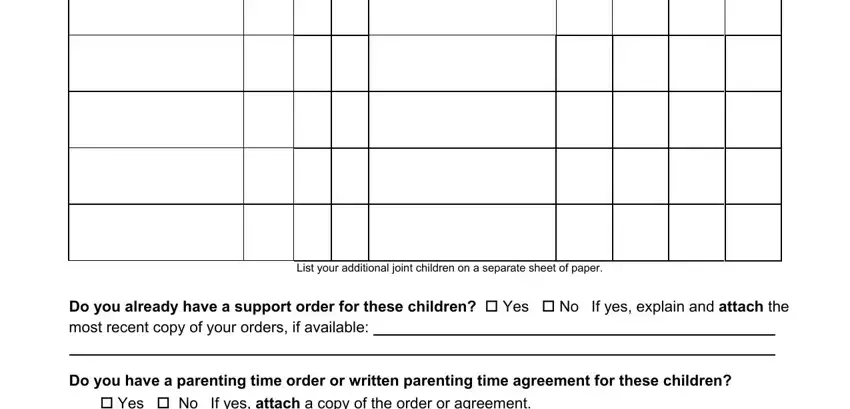
2. Soon after completing the last step, head on to the subsequent stage and complete all required details in all these blanks - List your additional joint, Do you already have a support, and Do you have a parenting time order.
3. The next part will be straightforward - fill out all of the fields in Do you support other children in, Childs First Name, Date of, Relationship, Birth, daughter son etc, If there is an order for you to, county court number, and Child in High School in Your Home to conclude this part.
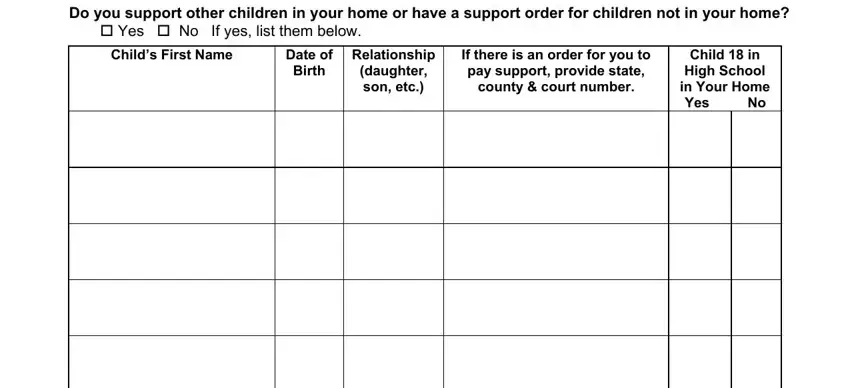
It is possible to make a mistake while filling out your Relationship, for that reason ensure that you take a second look before you submit it.
4. This next section requires some additional information. Ensure you complete all the necessary fields - List biological and adopted, Amount paid, Amount received, to whom, from whom, Are you employed Yes No, Name address phone number of, How many hours per week do you, Do you consistently receive wages, What is your monthly income before, Attach a copy of your most recent, Do you receive expense, Are you unemployed Yes No, Are you receiving workers, and If yes list the source and the - to proceed further in your process!
5. Because you come close to the completion of the document, you will find several more requirements that need to be met. Mainly, What type of work have you done in, Why did your last job end, Are you selfemployed Yes No, Name address phone number of your, Attach a copy of your most recent, and Page of UNIFORM INCOME EXPENSE must be filled in.
Step 3: After taking one more look at your fields, press "Done" and you're done and dusted! Sign up with FormsPal now and immediately use Form Csf 01 0100, prepared for download. Every modification made is conveniently preserved , so that you can modify the pdf at a later point when required. FormsPal is dedicated to the personal privacy of all our users; we ensure that all personal data used in our editor is confidential.