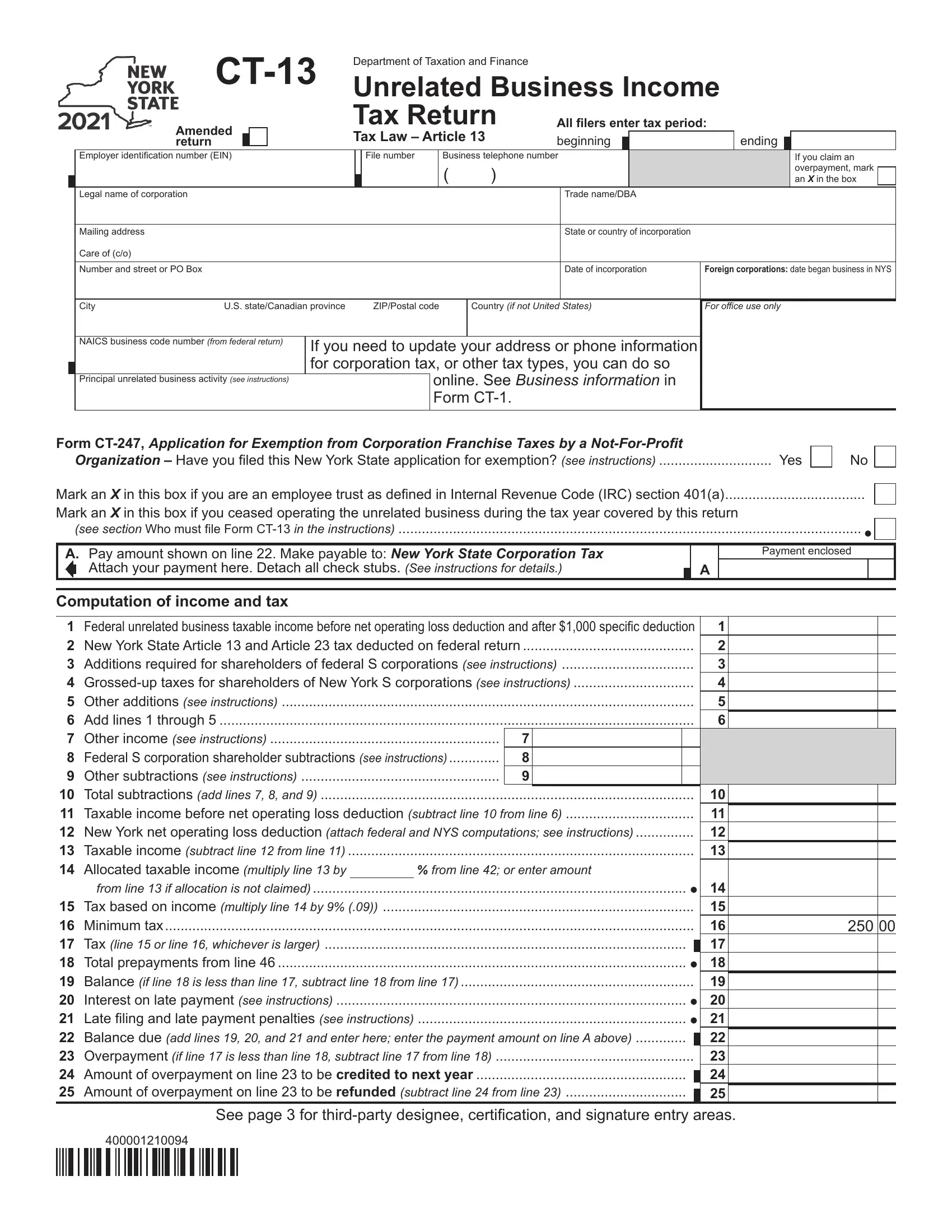
The Ct 13 form, officially known as the Unrelated Business Income Amended Tax Return, serves a crucial role for entities that need to amend their previously filed tax returns regarding unrelated business income in New York State. This comprehensive document requires filers to enter detailed information such as the tax period, Employer Identification Number (EIN), file number, business telephone number, legal name of the corporation, trade name or DBA, and mailing address, among other specifics. It is designed not only for the calculation and reporting of taxable income derived from business activities not related to the organization's exempt purpose but also to correct any errors or omissions in a previously filed Ct-13 form. The form demands a series of calculations to determine the amount of tax owed or the overpayment to be refunded or credited towards the next year. Additionally, it addresses situations like changes in operating status, allows filers to update contact information, and includes sections for reporting federal unrelated business taxable income adjustments, various New York State-specific additions and subtractions, allocated taxable income, and resulting taxes, emphasizing its importance in ensuring compliance and accuracy in tax filings for unrelated business income. Significantly, the form also provides spaces for third-party designee information, certification, and signatures, ensuring proper authorization and verification of the information provided.
| Question | Answer |
|---|---|
| Form Name | Form Ct 13 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | Form CT-13 Unrelated Business Income Tax Return Tax Year 2021 |
|
|
Department of Taxation and Finance |
|
|
|
|
|
|
|
|
||||||||||
|
|
Unrelated Business Income |
||||||||||||||||||
|
Amended |
|
|
|
|
Tax Return |
All filers enter tax period: |
|||||||||||||
|
|
|
|
|
Tax Law – Article 13 |
beginning |
|
|
|
ending |
|
|
||||||||
|
return |
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Employer identification number (EIN) |
|
|
File number |
|
Business telephone number |
|
|
|
|
|
If you claim an |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
overpayment, mark |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
an X in the box |
||
|
Legal name of corporation |
|
|
|
|
|
|
|
|
|
|
|
|
Trade name/DBA |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Mailing address |
|
|
|
|
|
|
|
|
|
|
|
|
State or country of incorporation |
|
|
|
|
||
|
Care of (c/o) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number and street or PO Box |
|
|
|
|
|
|
|
|
|
|
|
|
Date of incorporation |
Foreign corporations: date began business in NYS |
|||||
|
|
|
|
|
|
|
|
|
||||||||||||
|
City |
U.S. state/Canadian province |
|
ZIP/Postal code |
|
Country (if not United States) |
For office use only |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
NAICS business code number (from federal return) |
If you need to update your address or phone information |
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
for corporation tax, or other tax types, you can do so |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
online. See Business information in |
|
|
|
|
|||||||||
|
Principal unrelated business activity (see instructions) |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
Form |
|
|
|
|
|
|
|
|
|||
Form |
|
Organization – Have you filed this New York State application for exemption? (see instructions) |
Yes |
No
Mark an X in this box if you are an employee trust as defined in Internal Revenue Code (IRC) section 401(a)....................................
Mark an X in this box if you ceased operating the unrelated business during the tax year covered by this return
(see section Who must file Form
A.Pay amount shown on line 22. Make payable to: New York State Corporation Tax Attach your payment here. Detach all check stubs. (See instructions for details.)
A
Payment enclosed
Computation of income and tax
1 |
Federal unrelated business taxable income before net operating loss deduction and after $1,000 specific deduction |
1 |
||||||||
2 |
New York State Article 13 and Article 23 tax deducted on federal return |
............................................ |
|
|
|
2 |
||||
3 |
Additions required for shareholders of federal S corporations (see instructions) |
3 |
||||||||
4 |
4 |
|||||||||
5 |
Other additions (see instructions) |
|
|
|
|
|
5 |
|||
6 |
Add lines 1 through 5 |
|
|
|
|
|
6 |
|||
7 |
Other income (see instructions) |
|
7 |
|
|
|
|
|||
8 |
.............Federal S corporation shareholder subtractions (see instructions) |
|
8 |
|
|
|
|
|||
9 |
Other subtractions (see instructions) |
|
9 |
|
|
|
|
|||
10 |
................................................................................................Total subtractions (add lines 7, 8, and 9) |
|
|
|
|
|
10 |
|||
11 |
.................................Taxable income before net operating loss deduction (subtract line 10 from line 6) |
11 |
||||||||
12 |
New York net operating loss deduction (attach federal and NYS computations; see instructions) |
12 |
||||||||
13 |
Taxable income (subtract line 12 from line 11) |
|
|
|
|
|
13 |
|||
14 |
Allocated taxable income (multiply line 13 by |
|
|
% from line 42; or enter amount |
|
|||||
|
from line 13 if allocation is not claimed) |
|
|
|
|
|
14 |
|||
15 |
Tax based on income (multiply line 14 by 9% (.09)) |
|
|
|
|
|
15 |
|||
16 |
Minimum tax |
|
|
|
|
|
16 |
|||
17 |
Tax (line 15 or line 16, whichever is larger) |
|
|
|
|
|
|
17 |
||
|
|
|
|
|
||||||
18 |
Total prepayments from line 46 |
|
|
|
|
|
18 |
|||
19 |
............................................................Balance (if line 18 is less than line 17, subtract line 18 from line 17) |
|
|
|
19 |
|||||
20 |
Interest on late payment (see instructions) |
|
|
|
|
|
20 |
|||
21 |
Late filing and late payment penalties (see instructions) |
..................................................................... |
|
|
|
|
|
21 |
||
22 |
.............Balance due (add lines 19, 20, and 21 and enter here; enter the payment amount on line A above) |
22 |
||||||||
23 |
...................................................Overpayment (if line 17 is less than line 18, subtract line 17 from line 18) |
|
|
|
23 |
|||||
24 |
Amount of overpayment on line 23 to be credited to next year |
|
|
|
|
24 |
||||
|
|
|
||||||||
25 |
...............................Amount of overpayment on line 23 to be refunded (subtract line 24 from line 23) |
25 |
||||||||
|
|
|
|
|
|
|
|
|
|
|
250 00
See page 3 for
400001210094
Page 2 of 3
Have you been audited by the Internal Revenue Service in the past 5 years? Yes
No
If Yes, list years:
Federal return was filed on:
Other:
Attach a complete copy of your federal return.
Schedule A – Unrelated business allocation
If you did not maintain a regular place of business outside New York State, leave this schedule blank. A regular place of business is any office, factory, warehouse, or other space regularly used by the taxpayer in its unrelated business. If you
claim this allocation, attach a list of each place of business, the location, nature of activities, and number and duties of employees.
Average value of: |
|
A |
B |
|
|||
|
New York State |
Everywhere |
|
||||
26 |
Real estate owned (see instructions) |
26 |
|
|
|
|
|
27 |
Gross rents (attach list; see instructions) |
27 |
|
|
|
|
|
28 |
Inventories owned |
28 |
|
|
|
|
|
29 |
Other tangible personal property owned (see instructions) |
29 |
|
|
|
|
|
30 |
Total (add lines 26 through 29) |
30 |
|
|
|
|
|
31 |
Percentage in New York State (divide line 30, column A, by line 30, column B) |
31 |
|
% |
|||
Receipts in the regular course of business from:
32Sales of tangible personal property shipped to points within
|
New York State |
32 |
|
|
|
|
|
|
|
33 |
All sales of tangible personal property |
33 |
|
|
|
|
|
|
|
34 |
Services performed |
34 |
|
|
|
|
|
|
|
35 |
Rentals of property |
35 |
|
|
|
|
|
|
|
36 |
Other business receipts |
36 |
|
|
|
|
|
|
|
37 |
Total (add lines 32 through 36) |
37 |
|
|
|
|
|
|
|
38 |
Percentage in New York State (divide line 37, column A, by line 37, |
column B) |
|
|
38 |
|
|
% |
|
39Wages, salaries, and other compensation of employees
|
(except general executive officers; see instructions) |
39 |
|
|
|
|
|
|
|
|
40 |
Percentage in New York State (divide line 39, column A, by line 39, column B) |
|
|
|
40 |
|
% |
|||
41 |
Total of New York State percentages (add lines 31, 38, and 40) |
......................................................................... |
|
|
|
|
41 |
|
% |
|
42 |
Business allocation percentage (divide line 41 by three or by the number of percentages) |
........................................ |
|
|
|
42 |
|
% |
||
Composition of prepayments claimed on line 18* |
|
|
Date paid |
|
|
Amount |
||||
43 |
Payment with extension request, Form |
43 |
|
|
|
|
|
|
|
|
44a |
....................................................................Second installment from Form |
44a |
|
|
|
|
|
|
|
|
44b |
........................................................................Third installment from Form |
44b |
|
|
|
|
|
|
|
|
44c |
......................................................................Fourth installment from Form |
44c |
|
|
|
|
|
|
|
|
45 |
...............................................................................Amount of overpayment credited from prior years |
|
45 |
|
|
|
|
|
||
46 |
.....................................................Total prepayments (add lines 43 through 45; enter here and on line 18) |
46 |
|
|
|
|
|
|||
*Taxpayers subject to the unrelated business income tax are not required to make estimated tax payments. If you did make these unrequired payments, report them on lines 44a, 44b, and 44c.
Amended return information
If filing an amended return, mark an X in the box for any items that apply and attach documentation.
................Final federal determination |
If marked, enter date of determination: |
|
|
|
|
|
Capital loss carryback |
Federal return filed |
|
Form 1139 |
|||
Amended Form |
|
|
|
|
|
|
400002210094
Third – party |
Yes |
No |
Designee’s name (print) |
Designee’s phone number |
||
|
( |
) |
|
|||
designee |
|
|
|
|
|
|
Designee’s email address |
|
|
|
|||
|
PIN |
|||||
(see instructions) |
|
|
|
|
||
Certification: I certify that this return and any attachments are to the best of my knowledge and belief true, correct, and complete.
|
Printed name of authorized person |
|
Signature of authorized person |
|
Official title |
|
|||||
Authorized |
|
|
|
|
|
|
|
|
|
|
|
person |
Email address of authorized person |
|
|
|
Telephone number |
|
|
Date |
|
||
|
|
|
|
( |
) |
|
|
|
|
|
|
Paid |
Firm’s name (or yours if |
|
|
Firm’s |
EIN |
|
|
|
Preparer’s PTIN or SSN |
||
preparer |
|
|
|
|
|
|
|
|
|
|
|
use |
Signature of individual preparing this return |
Address |
City |
|
State |
ZIP code |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
only |
|
|
|
|
|
|
|
||||
Email address of individual preparing this return |
|
|
Preparer’s NYTPRIN or |
Excl. code Date |
|
||||||
(see instr.) |
|
|
|
|
|
|
|
|
|
|
|
See instructions for where to file.
400003210094