Navigating the intricacies of healthcare can often feel like moving through a maze, particularly when it involves ensuring that necessary medical services are accessible and covered under insurance programs such as Medicaid. An essential piece of this complex puzzle is the D 67 form, officially titled "Physician’s Medical Necessity Certification for Nonemergency Ambulance Transports." This form plays a pivotal role for patients who require nonemergency ambulance transportation—a service that might be needed when a patient's health condition prohibits them from using any other form of transportation to attend medical appointments. The form requires detailed information, including the patient's Medicaid number, transport dates, and a certification by a physician stating that the patient is severely disabled as defined by specific criteria set by the Medicaid Program. The stipulation that transportation must be medically necessary and reasonable sets a high bar for approval, underscoring the significance of the patient's condition and the physician’s attestation to their need for special transport. Additionally, the form covers various health conditions that would justify such nonemergency transports, ranging from the need for continuous oxygen or IV therapy to more extreme cases where the patient is comatose or requires trained monitoring. Beyond a mere administrative procedure, the completion and submission of the D 67 form are critical steps that ensure patients receive the care they need while also enabling healthcare providers to seek appropriate reimbursement from Medicaid, making it a crucial document in the healthcare continuum.
| Question | Answer |
|---|---|
| Form Name | Form D 67 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | TMPPM04, 2003, Necessity, HHSC |
Forms
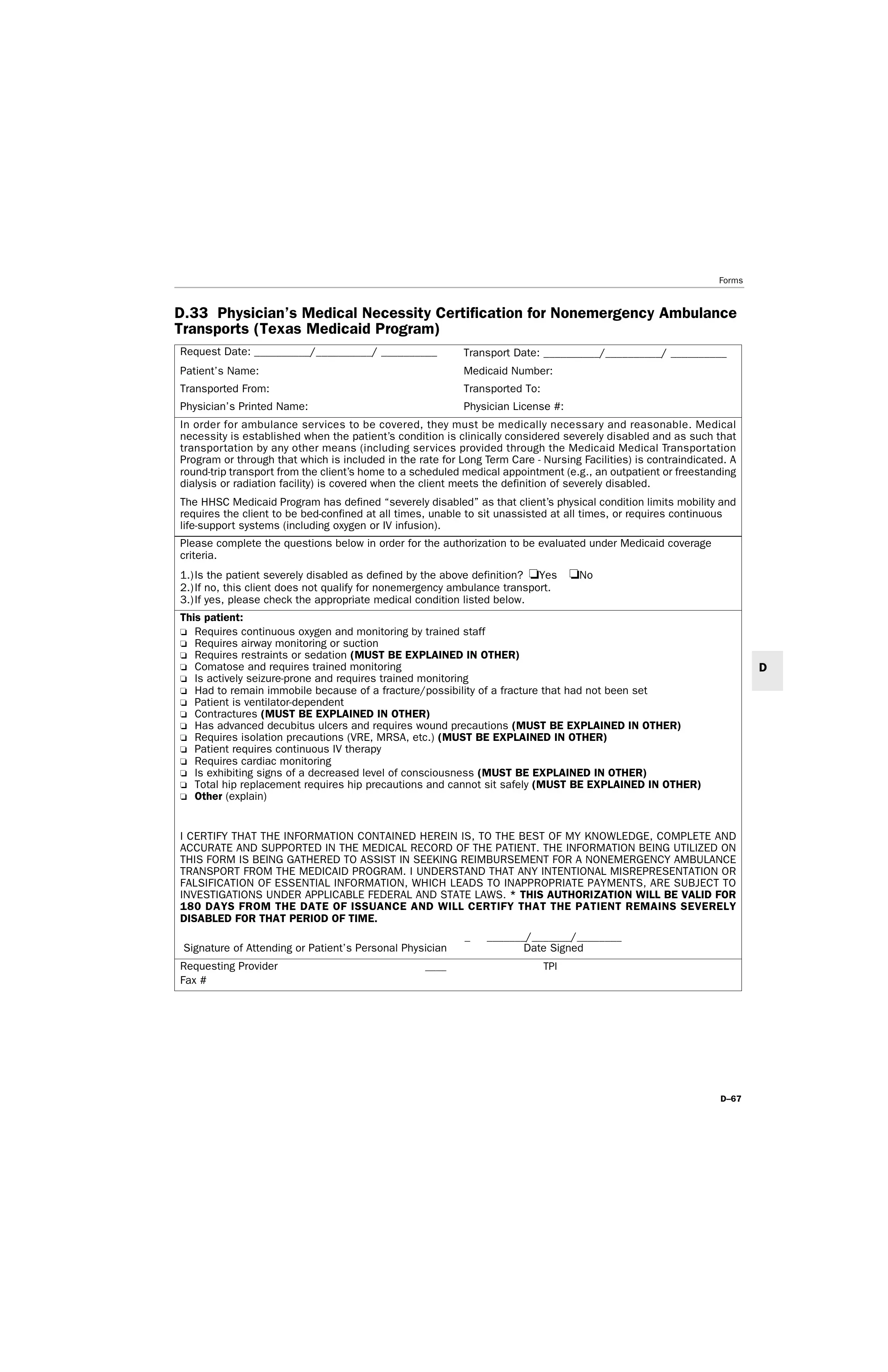
D.33 Physician’s Medical Necessity Certification for Nonemergency Ambulance Transports (Texas Medicaid Program)
Request Date: __________/__________/ __________ |
Transport Date: __________/__________/ __________ |
Patient’s Name: |
Medicaid Number: |
Transported From: |
Transported To: |
Physician’s Printed Name: |
Physician License #: |
In order for ambulance services to be covered, they must be medically necessary and reasonable. Medical necessity is established when the patient’s condition is clinically considered severely disabled and as such that transportation by any other means (including services provided through the Medicaid Medical Transportation Program or through that which is included in the rate for Long Term Care - Nursing Facilities) is contraindicated. A
The HHSC Medicaid Program has defined “severely disabled” as that client’s physical condition limits mobility and requires the client to be
Please complete the questions below in order for the authorization to be evaluated under Medicaid coverage criteria.
1.) Is the patient severely disabled as defined by the above definition? ❏Yes ❏No
2.) If no, this client does not qualify for nonemergency ambulance transport.
3.) If yes, please check the appropriate medical condition listed below.
This patient:
❏Requires continuous oxygen and monitoring by trained staff
❏Requires airway monitoring or suction
❏Requires restraints or sedation (MUST BE EXPLAINED IN OTHER)
❏Comatose and requires trained monitoring
❏Is actively
❏Had to remain immobile because of a fracture/possibility of a fracture that had not been set
❏Patient is
❏Contractures (MUST BE EXPLAINED IN OTHER)
❏Has advanced decubitus ulcers and requires wound precautions (MUST BE EXPLAINED IN OTHER)
❏Requires isolation precautions (VRE, MRSA, etc.) (MUST BE EXPLAINED IN OTHER)
❏Patient requires continuous IV therapy
❏Requires cardiac monitoring
❏Is exhibiting signs of a decreased level of consciousness (MUST BE EXPLAINED IN OTHER)
❏Total hip replacement requires hip precautions and cannot sit safely (MUST BE EXPLAINED IN OTHER)
❏Other (explain)
I CERTIFY THAT THE INFORMATION CONTAINED HEREIN IS, TO THE BEST OF MY KNOWLEDGE, COMPLETE AND ACCURATE AND SUPPORTED IN THE MEDICAL RECORD OF THE PATIENT. THE INFORMATION BEING UTILIZED ON THIS FORM IS BEING GATHERED TO ASSIST IN SEEKING REIMBURSEMENT FOR A NONEMERGENCY AMBULANCE TRANSPORT FROM THE MEDICAID PROGRAM. I UNDERSTAND THAT ANY INTENTIONAL MISREPRESENTATION OR FALSIFICATION OF ESSENTIAL INFORMATION, WHICH LEADS TO INAPPROPRIATE PAYMENTS, ARE SUBJECT TO INVESTIGATIONS UNDER APPLICABLE FEDERAL AND STATE LAWS. * THIS AUTHORIZATION WILL BE VALID FOR 180 DAYS FROM THE DATE OF ISSUANCE AND WILL CERTIFY THAT THE PATIENT REMAINS SEVERELY DISABLED FOR THAT PERIOD OF TIME.
|
|
_ _______/_______/________ |
Signature of Attending or Patient’s Personal Physician |
Date Signed |
|
|
|
|
Requesting Provider |
____ |
TPI |
Fax # |
|
|
D