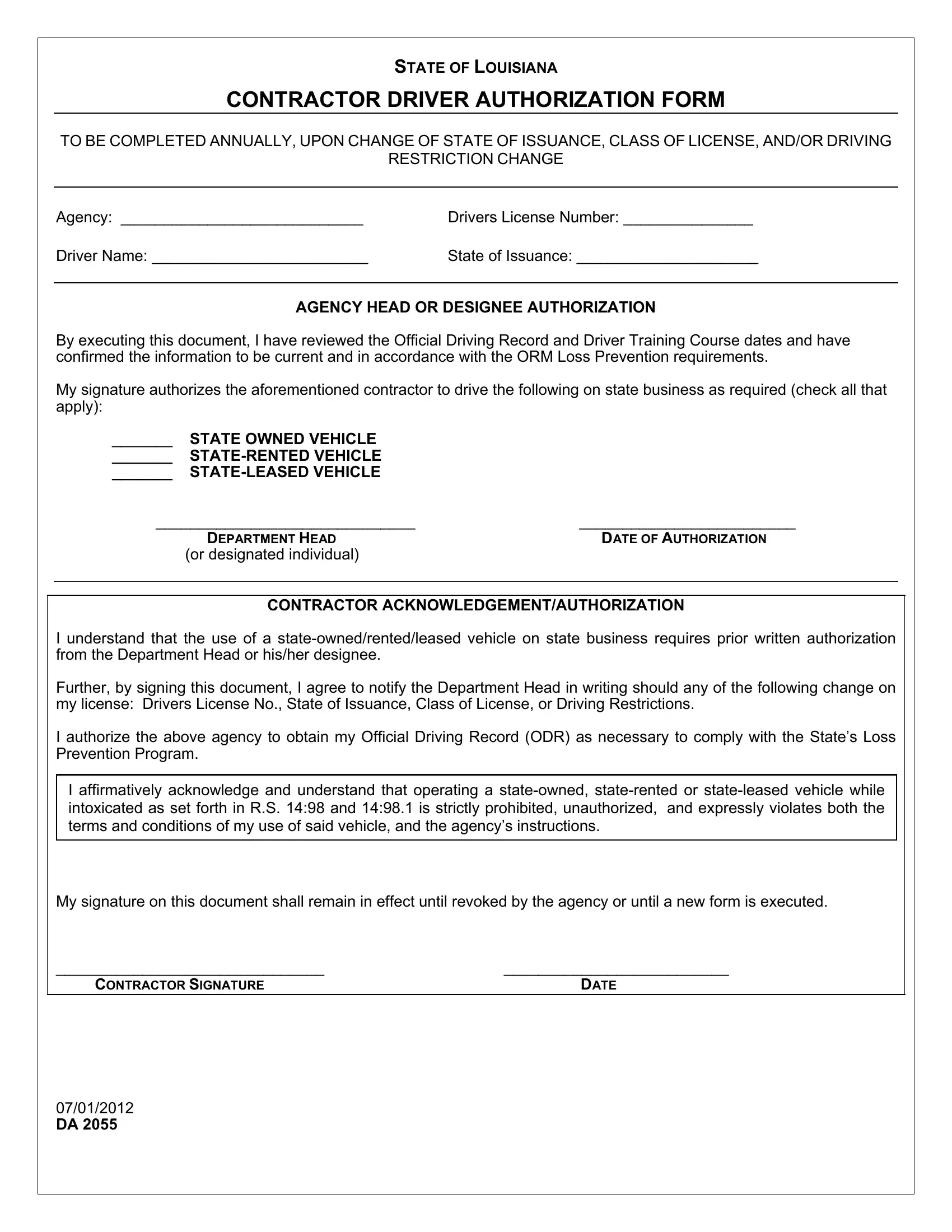
Every year, or whenever there's a change in their driving credentials, contractors in Louisiana must complete the Contractor Driver Authorization Form, also known as the DA form. This requirement is essential for any contractor who drives a state-owned, rented, or leased vehicle as part of their duties. The form collects basic information such as the agency name, the driver's license number, the driver's name, and the state where the license was issued. It also includes a section for the agency head or their designee to authorize the contractor's driving privileges, affirming that they have reviewed the driver's official record and training course dates to ensure compliance with the Office of Risk Management (ORM) Loss Prevention requirements. Contractors, on their part, promise to notify the department head of any changes to their driving license details and acknowledge the prohibition against operating the vehicle under the influence. The form, which needs to be signed by both the contractor and the agency head or designated individual, plays a crucial role in maintaining safety and compliance within state business operations, embodying a systematic approach to risk management and accountability.
| Question | Answer |
|---|---|
| Form Name | Form Da 2055 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ISSUANCE, ORM, authorization to release vehicle louisiana, vehicle release form dmv |
STATE OF LOUISIANA
CONTRACTOR DRIVER AUTHORIZATION FORM
TO BE COMPLETED ANNUALLY, UPON CHANGE OF STATE OF ISSUANCE, CLASS OF LICENSE, AND/OR DRIVING
RESTRICTION CHANGE
Agency: ____________________________ |
Drivers License Number: _______________ |
Driver Name: _________________________ |
State of Issuance: _____________________ |
AGENCY HEAD OR DESIGNEE AUTHORIZATION
By executing this document, I have reviewed the Official Driving Record and Driver Training Course dates and have confirmed the information to be current and in accordance with the ORM Loss Prevention requirements.
My signature authorizes the aforementioned contractor to drive the following on state business as required (check all that apply):
_______ |
STATE OWNED VEHICLE |
|
_______ |
|
|
_______ |
|
|
______________________________ |
_________________________ |
|
|
DEPARTMENT HEAD |
DATE OF AUTHORIZATION |
|
(or designated individual) |
|
CONTRACTOR ACKNOWLEDGEMENT/AUTHORIZATION
I understand that the use of a
Further, by signing this document, I agree to notify the Department Head in writing should any of the following change on my license: Drivers License No., State of Issuance, Class of License, or Driving Restrictions.
I authorize the above agency to obtain my Official Driving Record (ODR) as necessary to comply with the State’s Loss Prevention Program.
I affirmatively acknowledge and understand that operating a
My signature on this document shall remain in effect until revoked by the agency or until a new form is executed.
_______________________________ |
__________________________ |
CONTRACTOR SIGNATURE |
DATE |
07/01/2012
DA 2055
ANNUAL SUPPLEMENTAL SIGNATURE PAGE
CONTRACTOR NAME:_____________________________
DRIVERS LICENSE NUMBER:_______________________
DEPARTMENT/AGENCY:___________________________
AGENCY HEAD OR DESIGNEE STATEMENT
By executing this document, I have reviewed the following and have confirmed the information to be current and in accordance with the ORM Loss Prevention requirement:
Official Driving Record
Further, my signature allows the aforementioned contractor to drive a
______________________________ |
_________________________ |
Agency Head |
Date of Authorization |
(or designated individual) |
|
______________________________ |
_________________________ |
Agency Head |
Date of Authorization |
(or designated individual) |
|
______________________________ |
_________________________ |
Agency Head |
Date of Authorization |
(or designated individual) |
|
______________________________ |
_________________________ |
Agency Head |
Date of Authorization |
(or designated individual) |
|
______________________________ |
_________________________ |
Agency Head |
Date of Authorization |
(or designated individual) |
|
______________________________ |
_________________________ |
Agency Head |
Date of Authorization |
(or designated individual) |
|
______________________________ |
_________________________ |
Agency Head |
Date of Authorization |
(or designated individual) |
|
(DUPLICATE SUPPLEMENTAL SIGNATURE PAGE AS NEEDED)
07/01/2012
DA 2055