








 Yes
Yes 
 No
No

We were designing this PDF editor with the prospect of allowing it to be as quick make use of as possible. This is the reason the process of completing the form db 450 is going to be effortless as you go through these actions:
Step 1: The first thing is to select the orange "Get Form Now" button.
Step 2: At this point, you are on the document editing page. You can add content, edit current data, highlight specific words or phrases, place crosses or checks, insert images, sign the file, erase unnecessary fields, etc.
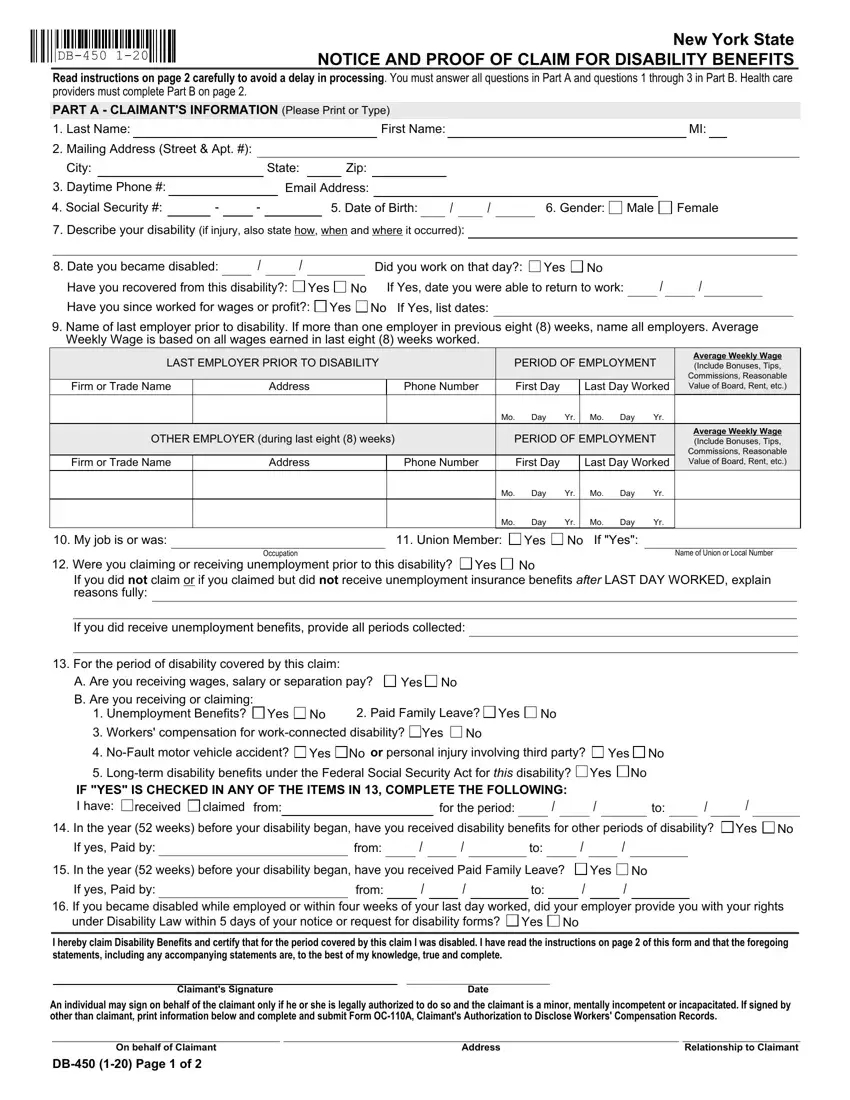
Provide the necessary details in every segment to fill in the PDF form db 450
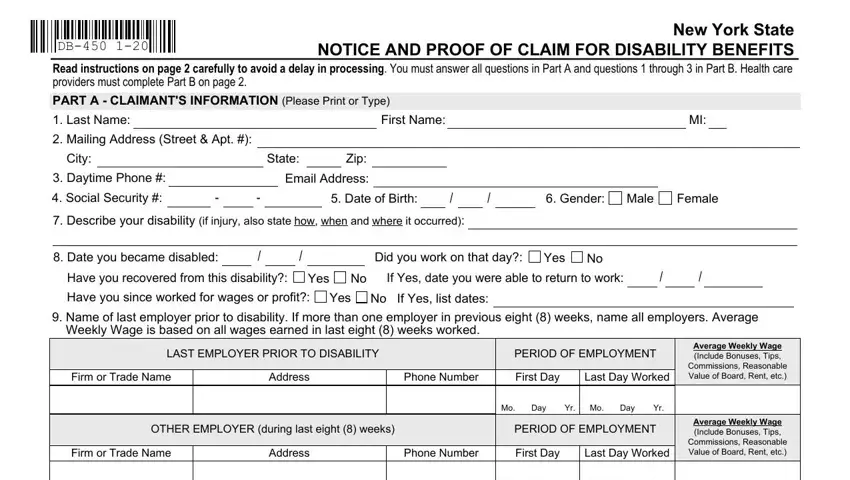
Enter the demanded particulars in My job is or was, Union Member, Yes, If Yes, Occupation, Name of Union or Local Number, Were you claiming or receiving, Yes, If you did not claim or if you, Mo Day Yr, Mo Day Yr, Mo Day Yr, Mo Day Yr, If you did receive unemployment, and For the period of disability box.
Inside the section referring to I hereby claim Disability Benefits, An individual may sign on behalf, Claimants Signature, Date, On behalf of Claimant, DB Page of, Address, and Relationship to Claimant, make sure you note some significant data.

The PART B HEALTH CARE PROVIDERS, Last Name, First Name, Gender, Male, Female, Date of Birth, DiagnosisAnalysis, a Claimants symptoms, b Objective findings, Diagnosis Code, Claimant hospitalized, Operation indicated, Yes, and Yes box will be your place to put the rights and obligations of each party.
Finalize by taking a look at all these areas and preparing them correspondingly: Health Care Providers Printed Name, Health Care Providers Signature, Date, Health Care Providers Address, Phone, IMPORTANT NOTICE TO CLAIMANT READ, PLEASE NOTE Do not date and file, If you are using this form, If you are using this form, If you do not receive a response, Notification Pursuant to the New, and HIPAA NOTICE In order to.
Step 3: Select the Done button to save the document. Now it is at your disposal for transfer to your gadget.
Step 4: To protect yourself from probable upcoming concerns, you should get as much as a pair of copies of each document.
