The DCSS S147 form is a cornerstone for those receiving child support in New Hampshire, providing a streamlined and secure method to receive payments directly into a bank account, thus eliminating the wait times and insecurity associated with traditional checks. This form, officially titled the Child Support Direct Deposit Authorization Agreement, is issued by the New Hampshire Department of Health & Human Services. It is designed for individuals to either sign up for direct deposit of child support payments for the first time or to request changes to an existing direct deposit setup. To facilitate a smooth transaction, the applicant is required to provide detailed information including personal identification, bank account details, and a certification that acknowledges understanding and agreement to the terms detailed on the form. Moreover, applicants opting for the direct deposit into a checking account must include a voided check to confirm their bank account details. The importance of keeping the New Hampshire Division of Child Support Services updated with any changes in address is underscored to prevent any disruptions in the direct deposit service. Additionally, the form outlines procedures for changing financial institutions, canceling the service, and the legal ramifications of providing false information. This meticulous process ensures both the security of the financial transactions involved and the reliable delivery of child support payments, demonstrating a commitment to the welfare of the beneficiaries.
| Question | Answer |
|---|---|
| Form Name | Form Dcss S147 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | directdeposit printable child support form for new hampshire |
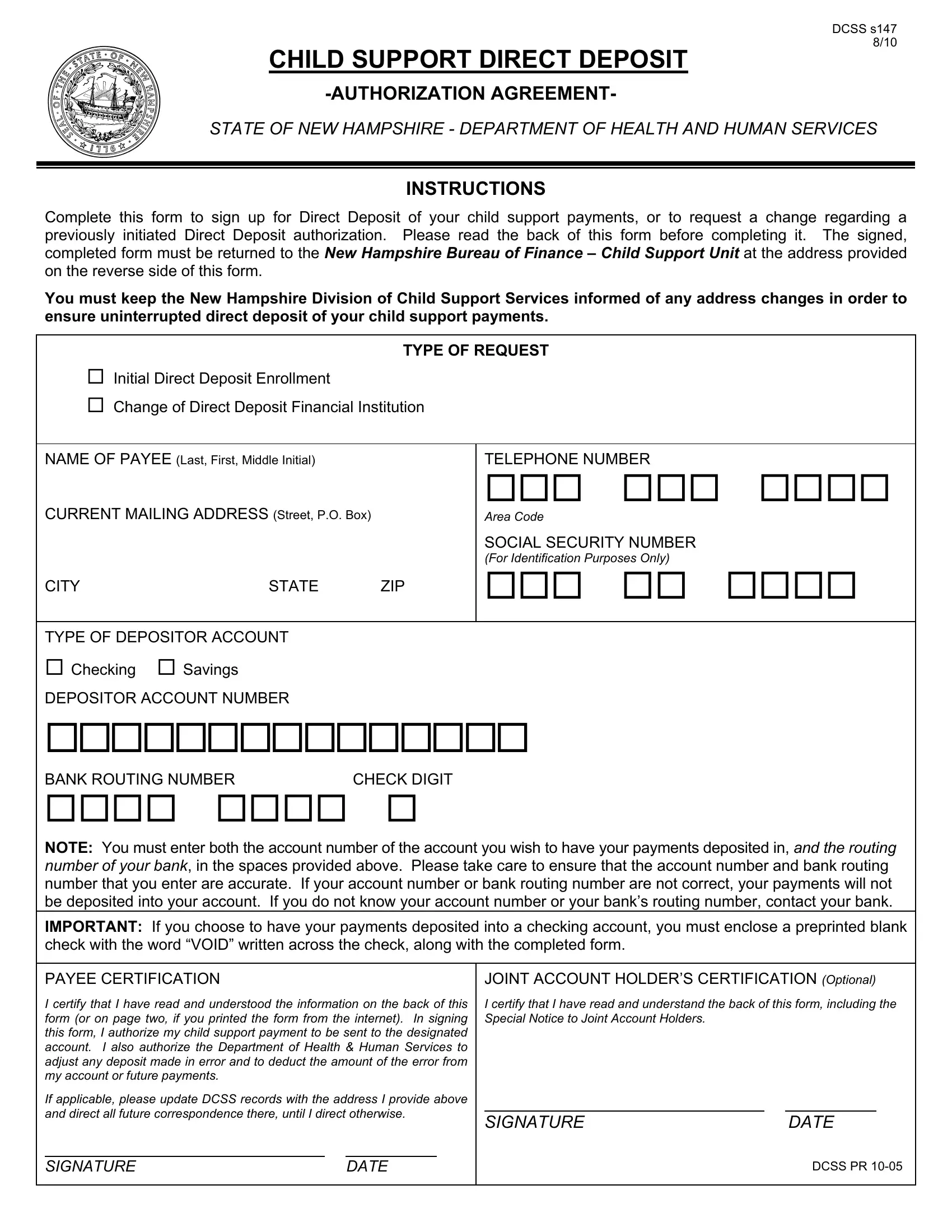
DCSS s147 8/10
CHILD SUPPORT DIRECT DEPOSIT
STATE OF NEW HAMPSHIRE - DEPARTMENT OF HEALTH AND HUMAN SERVICES
INSTRUCTIONS
Complete this form to sign up for Direct Deposit of your child support payments, or to request a change regarding a previously initiated Direct Deposit authorization. Please read the back of this form before completing it. The signed, completed form must be returned to the New Hampshire Bureau of Finance – Child Support Unit at the address provided on the reverse side of this form.
You must keep the New Hampshire Division of Child Support Services informed of any address changes in order to ensure uninterrupted direct deposit of your child support payments.
|
|
TYPE OF REQUEST |
|
Initial Direct Deposit Enrollment |
|
|
|
Change of Direct Deposit Financial Institution |
|
||
|
|
|
|
NAME OF PAYEE (Last, First, Middle Initial) |
|
TELEPHONE NUMBER |
|
CURRENT MAILING ADDRESS (Street, P.O. Box) |
Area Code |
||
|
|
|
SOCIAL SECURITY NUMBER |
|
|
|
(For Identification Purposes Only) |
CITY |
STATE |
ZIP |
|
|
|
|
|
TYPE OF DEPOSITOR ACCOUNT |
|
|
|
Checking |
Savings |
|
|
DEPOSITOR ACCOUNT NUMBER |
|
|
|
BANK ROUTING NUMBER |
CHECK DIGIT |
|
|
NOTE: You must enter both the account number of the account you wish to have your payments deposited in, and the routing number of your bank, in the spaces provided above. Please take care to ensure that the account number and bank routing number that you enter are accurate. If your account number or bank routing number are not correct, your payments will not be deposited into your account. If you do not know your account number or your bank’s routing number, contact your bank.
IMPORTANT: If you choose to have your payments deposited into a checking account, you must enclose a preprinted blank check with the word “VOID” written across the check, along with the completed form.
|
PAYEE CERTIFICATION |
|
|
|
|
JOINT ACCOUNT HOLDER’S CERTIFICATION (Optional) |
|||
|
I certify that I have read and understood the information on the back of this |
|
I certify that I have read and understand the back of this form, including the |
||||||
|
form (or on page two, if you printed the form from the internet). In signing |
|
Special Notice to Joint Account Holders. |
|
|
|
|||
|
this form, I authorize my child support payment to be sent to the designated |
|
|
|
|
|
|||
|
account. I also authorize the Department of Health & Human Services to |
|
|
|
|
|
|||
|
adjust any deposit made in error and to deduct the amount of the error from |
|
|
|
|
|
|||
|
my account or future payments. |
|
|
|
|
|
|
|
|
|
If applicable, please update DCSS records with the address I provide above |
|
|
|
|
|
|||
|
and direct all future correspondence there, until I direct otherwise. |
|
|
|
|
|
|||
|
SIGNATURE |
|
DATE |
||||||
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE |
|
DATE |
|
|
|
DCSS PR |
||
|
|
|
|
|
|
|
|
|
|
DIRECT
DEPOSIT
•FASTER AND EASIER ACCESS TO
YOUR CHILD SUPPORT
•NO MORE LOST OR STOLEN CHECKS
•NO MORE LONG BANK LINES
WHAT IS DIRECT DEPOSIT?
Direct deposit is also known as electronic funds transfer (EFT). As a recipient of child support services you can authorize the New Hampshire Department of Health & Human Services (DHHS) to deposit your child support payments directly into your account.
HOW DOES IT WORK?
When a payment is posted to your child support case, DHHS electronically tells your bank to credit your account. In most instances, the payment will be received at your bank within two business days after DHHS disburses the payment.
HOW DO I SIGN UP FOR DIRECT DEPOSIT?
To ensure that only authorized individuals see your account information, please complete the authorization agreement on the reverse side according to directions and mail the original form to the New Hampshire Bureau of Finance - Child Support Unit at the following address:
Department of Health & Human Services
Bureau of Finance - Child Support Unit (DDP)
129 Pleasant Street
Concord NH
__________________________________________________________________________________________________________________________________________________________________________________________________________
The information on the back of this form will be used to process payment data from the Department of Health & Human Services to the financial institution and/or its agent. Failure to provide the requested information may affect the processing of this form and may delay or prevent the receipt of payments through the Direct Deposit Program.
ACCESS TO ACCOUNT
Once the direct deposit is electronically completed, any questions regarding access to the funds are between the payee and the financial institution. All inquiries and liabilities regarding access to funds must be addressed to the financial institution.
SPECIAL NOTICE TO JOINT ACCOUNT HOLDERS
Joint account holders should immediately advise both the Department of Health & Human Services and the financial institution of the death of an account holder. Funds deposited after the date of death or ineligibility of the Child Support payee are to be returned to the Department of Health & Human Services. Each joint account holder hereby irrevocably directs the financial institution, upon notice and request of the Department of Health & Human Services, to return such funds to the Department of Health & Human Services. The financial institution will be held harmless by the Department of Health & Human Services for any claim arising in connection with this procedure.
CANCELLATION
The agreement represented by this authorization remains in effect until cancelled by the recipient by written notice to the Department of Health & Human Services or by death or legal incapacity of the recipient. Upon cancellation by the recipient, the recipient should notify the receiving financial institution that she/he is doing so. The agreement is deemed to be cancelled upon the closing of the account in the financial institution.
The agreement represented by this authorization may be cancelled by the financial institution by providing the payee a written notice postmarked 30 days in advance of the cancellation date to the address listed on the account. The payee must immediately advise the Department of Health & Human Services if direct deposit is to be cancelled by the financial institution. The financial institution cannot cancel the authorization solely by advice to the Department of Health & Human Services.
CHANGING RECEIVING FINANCIAL INSTITUTIONS
The payee’s direct deposit will continue to be received by the selected financial institution until cancelled in writing as provided above, or until the Department of Health & Human Services and the financial institution are notified by the payee (in writing) that the payee wishes to change the financial institution that is receiving direct deposit. In addition, the payee will complete a new copy of this form with the newly selected financial institution. It is recommended that the payee maintain both accounts at both financial institutions until the transition is complete, i.e., after the new financial institution received the payee’s first direct deposit payment.
FALSE STATEMENTS OR FRAUDULENT CLAIMS
State law provides a fine of not more than $2,000 or imprisonment for not more than one (1) year or both for giving false information in connection with making a written or electronic false statement that the party does not believe to be true (NH RSA 651:2 and 641:3).