

The Arizona DD-191-FF form maintains complete records of events, including accidents, injuries, or any significant occurrences that need review or further action. Here's a detailed guide on filling out this document.
1. Fill in Personal Information
Begin by writing the individual's name, Focus ID number, birth date, and complete address.
2. Incident Details
Provide the name and location of the incident, including the site name and address. Specify the date and time of the incident, choosing AM or PM as appropriate.
3. Provider Information
If the incident occurred under the supervision of a provider, state the provider's name at the time of the incident. This could be a qualified vendor, an individual independent provider, or the name of the provider site.
4. Staff and Witness Information
List the names of any staff or witnesses involved, along with their phone numbers. If applicable, include their immediate supervisors.
5. Describe the Incident
Detail what happened before, during, and after the incident. Be clear, objective, and chronological in your description. Avoid personal opinions to maintain the report's objectivity.
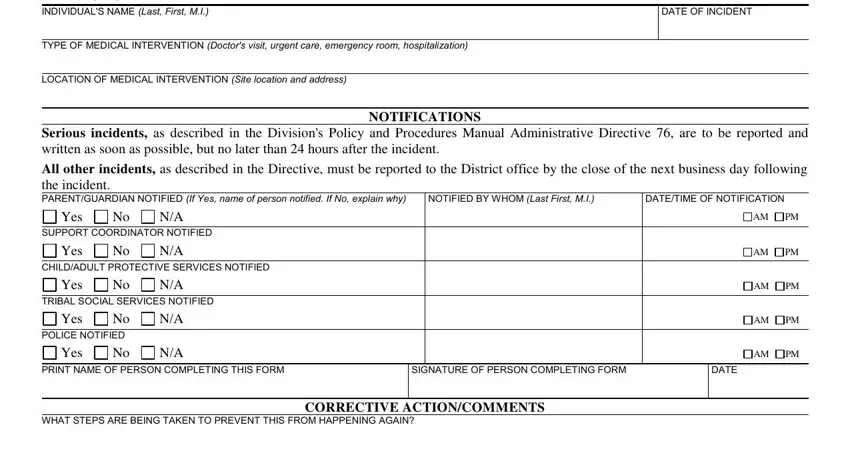
6. Medical Intervention
If medical intervention was necessary, note the type (e.g., doctor's visit, hospitalization) and the location of the medical intervention.

7. Notifications
Record details about notifications made to parents or guardians, support coordinators, and other relevant parties such as Child/Adult Protective Services or police. Specify who made the notification, the date, and time.
8. Completing the Form
The person completing the form must print their name, sign, and date it. If corrective actions are suggested to prevent future incidents, these should be described under the "Corrective Action/Comments" section. Finally, the supervisor should print their name, sign, and date the form to confirm the information and the follow-up actions.