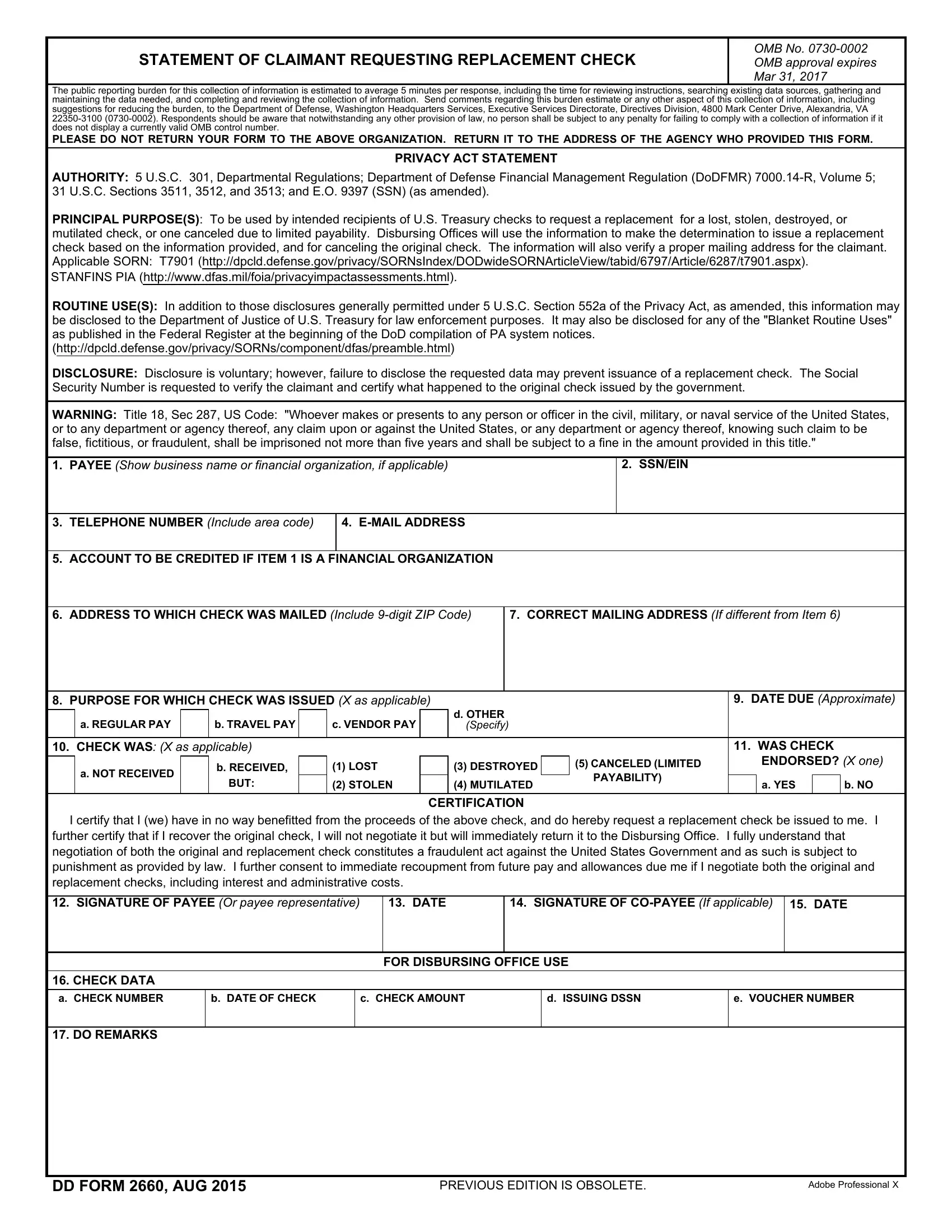

When working in the online PDF editor by FormsPal, you can easily complete or change dd form 2660 pdf here. In order to make our tool better and easier to utilize, we consistently develop new features, considering suggestions coming from our users. To start your journey, consider these simple steps:
Step 1: Open the PDF form in our tool by clicking the "Get Form Button" in the top part of this page.
Step 2: With our advanced PDF tool, it is easy to accomplish more than simply fill in blank fields. Try all the functions and make your documents seem sublime with customized text incorporated, or optimize the original input to perfection - all that comes with an ability to insert almost any pictures and sign the document off.
Completing this form calls for care for details. Ensure that every blank is completed correctly.
1. To start off, while completing the dd form 2660 pdf, start in the section that contains the next blanks:
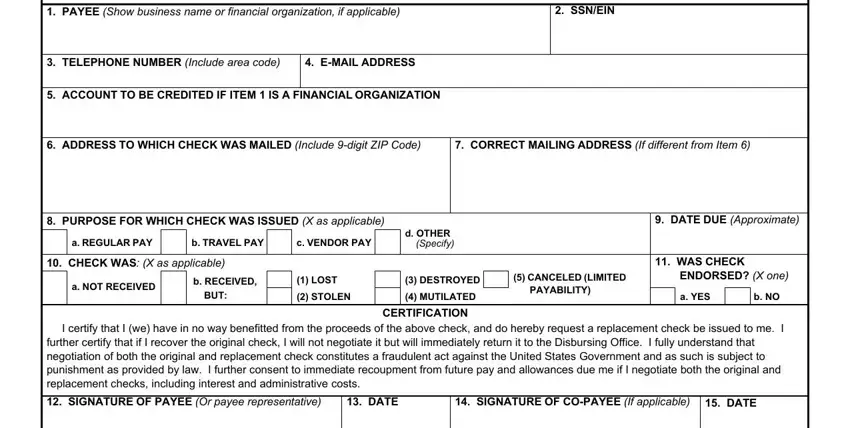
2. Now that the previous array of fields is complete, you're ready add the essential specifics in b DATE OF CHECK, c CHECK AMOUNT, d ISSUING DSSN, e VOUCHER NUMBER, CHECK DATA a CHECK NUMBER, DO REMARKS, DD FORM AUG, PREVIOUS EDITION IS OBSOLETE, and Adobe Professional X so you're able to proceed to the next part.
It is easy to get it wrong while filling in your b DATE OF CHECK, consequently be sure you look again before you decide to finalize the form.
Step 3: After you've looked again at the details in the document, simply click "Done" to finalize your FormsPal process. Acquire the dd form 2660 pdf as soon as you join for a 7-day free trial. Immediately use the pdf document inside your FormsPal account, along with any edits and adjustments being automatically saved! FormsPal is devoted to the personal privacy of our users; we ensure that all personal information handled by our system continues to be protected.