
To complete your CRSC (Combat-Related Special Compensation) DD Form 2860 online, no downloads or software installations are needed. Army, Navy, Marine Corps, Air Force, and Coast Guard retirees with combat-related disability ratings can use our free PDF tool to fill out and submit the application. Here is how to get started:
Step 1: Open the CRSC application PDF in our tool by clicking the "Get Form Button" at the top of this page.
Step 2: Our tool lets you customize nearly all PDF documents in many different ways. Edit your CRSC application by adding personalized text, adjusting existing content, and adding a digital signature, all in minutes.
As for the blanks of this particular document, here is what you need to do:
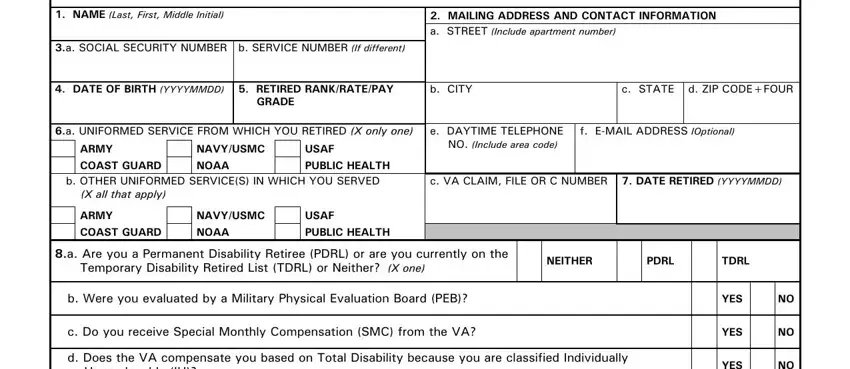
1. Whenever filling in the CRSC application, make certain to complete all important blanks in each relevant section. This will help expedite the review process, allowing your disability details to be handled efficiently and correctly.
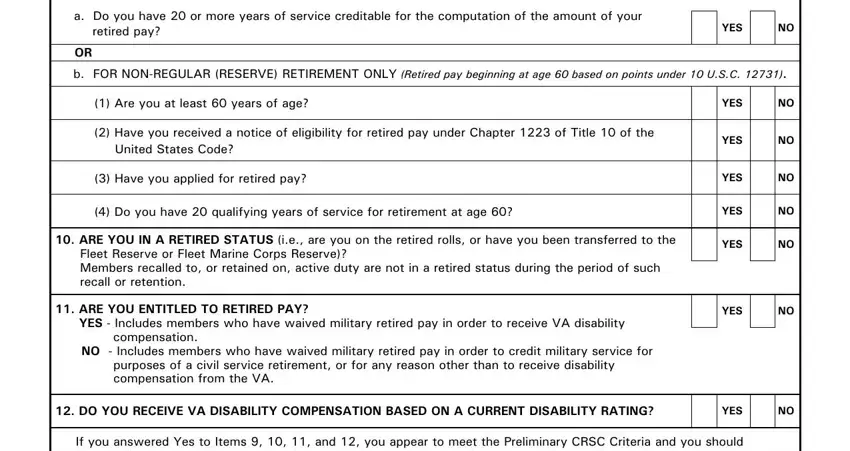
2. Once your current task is complete, take the next step and fill out all of these fields: a Do you have or more years of, YES, b FOR NONREGULAR RESERVE, Are you at least years of age, Have you received a notice of, Have you applied for retired pay, Do you have qualifying years of, ARE YOU IN A RETIRED STATUS ie, ARE YOU ENTITLED TO RETIRED PAY, YES, YES, YES, YES, YES, and YES with their corresponding information. Make sure to double check that everything has been entered correctly before continuing.
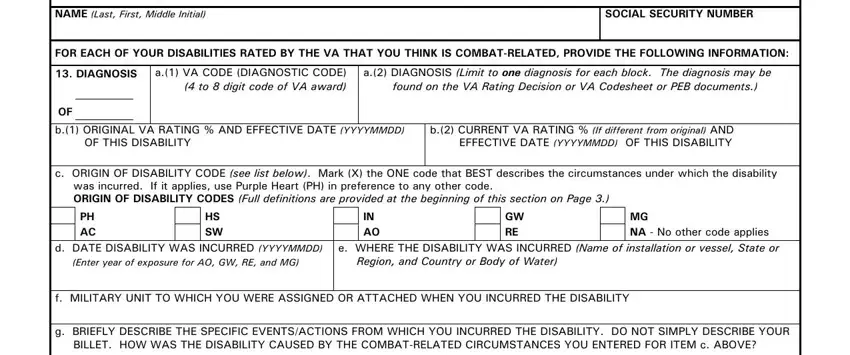
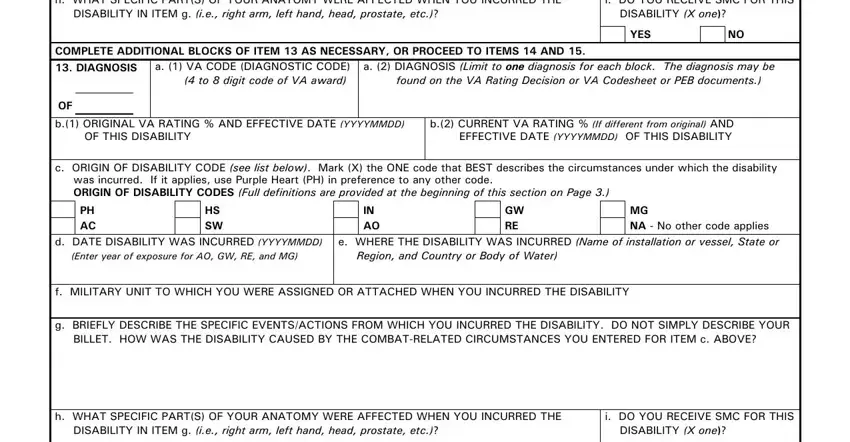
3. Within this stage, review If you are unable to answer any of, SOCIAL SECURITY NUMBER, FOR EACH OF YOUR DISABILITIES, DIAGNOSIS, a VA CODE DIAGNOSTIC CODE to, a DIAGNOSIS Limit to one diagnosis, OF b ORIGINAL VA RATING AND, b CURRENT VA RATING If different, c ORIGIN OF DISABILITY CODE see, PH AC, HS SW, IN AO, GW RE, MG NA No other code applies, and d DATE DISABILITY WAS INCURRED. All these must be filled in with utmost accuracy for your CRSC disability claim.
4. This next section requires some additional information. Ensure you complete all the necessary fields: h WHAT SPECIFIC PARTS OF YOUR, i DO YOU RECEIVE SMC FOR THIS, YES, COMPLETE ADDITIONAL BLOCKS OF ITEM, a VA CODE DIAGNOSTIC CODE to, a DIAGNOSIS Limit to one, OF b ORIGINAL VA RATING AND, b CURRENT VA RATING If different, c ORIGIN OF DISABILITY CODE see, PH AC, HS SW, IN AO, GW RE, MG NA No other code applies, and d DATE DISABILITY WAS INCURRED to proceed further in your CRSC process.
Always be really mindful while completing i DO YOU RECEIVE SMC FOR THIS and GW RE, as this is where a lot of people make some mistakes in their CRSC application.
5. This document needs to be completed by filling in this section. Further you can find a comprehensive list of blank fields: DD FORM TEST V APR, YES, Page, and of Pages. Completing this final section correctly ensures your CRSC combat-related disability claim is submitted in full.

Step 3: Once you have reviewed all the details in the blanks, click "Done" to finalize your CRSC application. You can then download, print, or share the completed DD Form 2860 Test directly from FormsPal. Every change is saved automatically, so you can return to edit your CRSC application at any time if needed. Your personal disability information is kept protected throughout the process.
Need related military forms? Visit these pages for additional assistance: DD Form 2656 for retirement pay elections, Disability Claim Form for veterans benefit documentation, and Veterans Affair Attendant Affidavit for caregiving support.