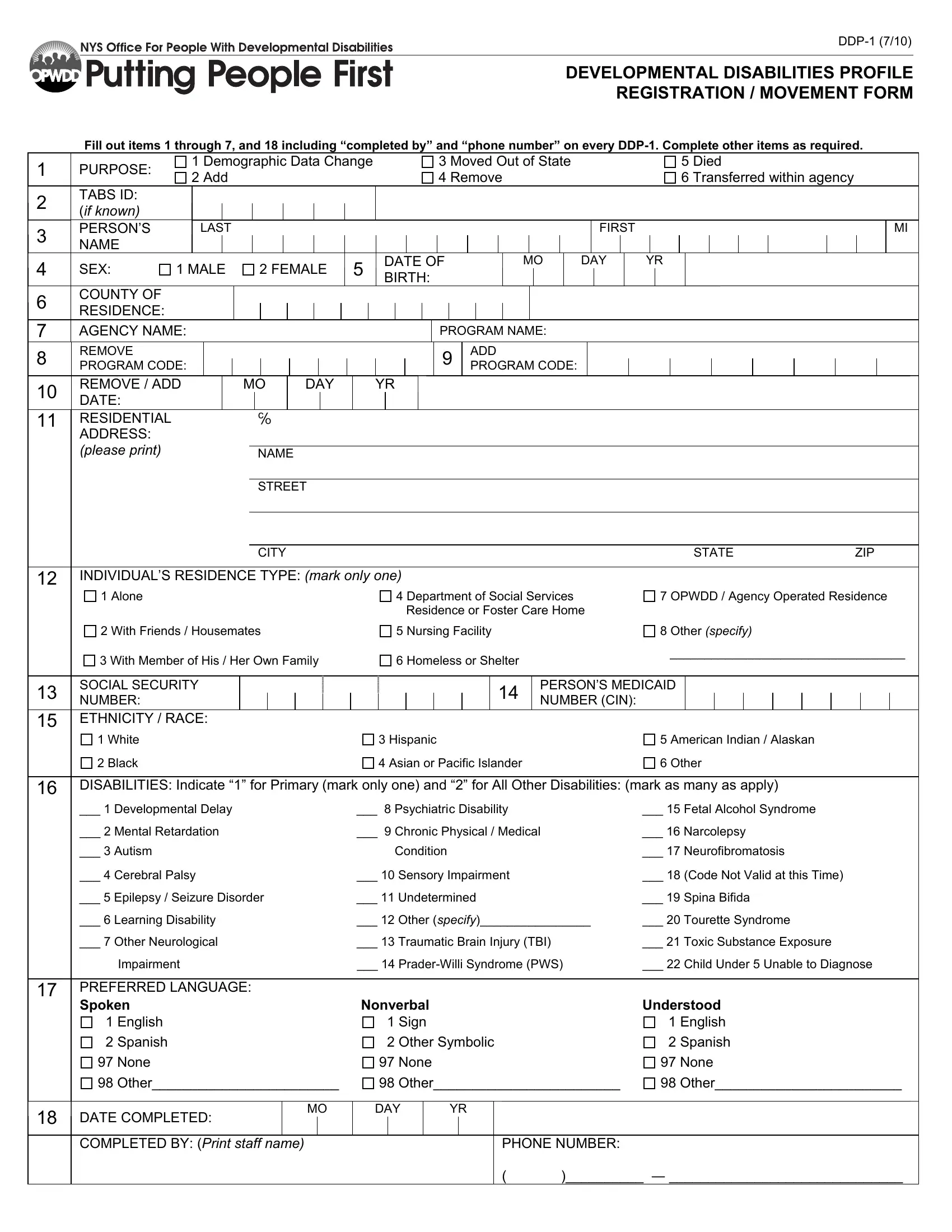
In an evolving landscape where the administration and management of programs services for individuals with developmental disabilities remain paramount, the Developmental Disabilities Profile Registration/Movement Form, known colloquially as the DDP-1, emerges as a critical tool. This form is meticulously designed to collect essential demographic, residential, and programmatic information for individuals receiving services under the umbrella of agencies certified or funded by the Office for People With Developmental Disabilities (OPWDD). Mandating completion of specific items such as demographic data, the individual's name, sex, date of birth, and county of residence, the DDP-1 ensures that vital information is systematically recorded and updated. Moreover, it encompasses a broad spectrum of purposes including changes in demographic data, additions, removals, transfers within the agency, out-of-state moves, and death notifications. Program codes, an eight-digit number crucial for program identification within the TABS system, along with preferred communication methods and officially documented disabilities, stand out as indispensable elements in aligning individuals with the most appropriate and responsive services. Through the structured completion of items 1-7 and 18 by agency staff, the DDP-1 form acts as a linchpin in the overarching goal of delivering tailored and efficacious services to those with developmental disabilities, ensuring their needs are met with precision and understanding.
| Question | Answer |
|---|---|
| Form Name | Form DDP-1 |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 24 |
| Avg. time to fill out | 5 min 7 sec |
| Other names | prader, Neurofibromatosis, DDP, ddp1 |