

Using PDF files online is always super easy with our PDF editor. Anyone can fill in form 224 here within minutes. FormsPal team is focused on providing you the ideal experience with our editor by continuously introducing new features and enhancements. With these updates, using our editor gets easier than ever! If you are looking to get going, here is what you will need to do:
Step 1: Simply click on the "Get Form Button" at the top of this site to launch our form editing tool. This way, you will find all that is needed to work with your file.
Step 2: As you open the PDF editor, you will find the document made ready to be completed. Apart from filling in various blank fields, it's also possible to do other things with the file, such as putting on your own text, editing the original textual content, inserting images, placing your signature to the form, and much more.
As for the blank fields of this precise form, this is what you should do:
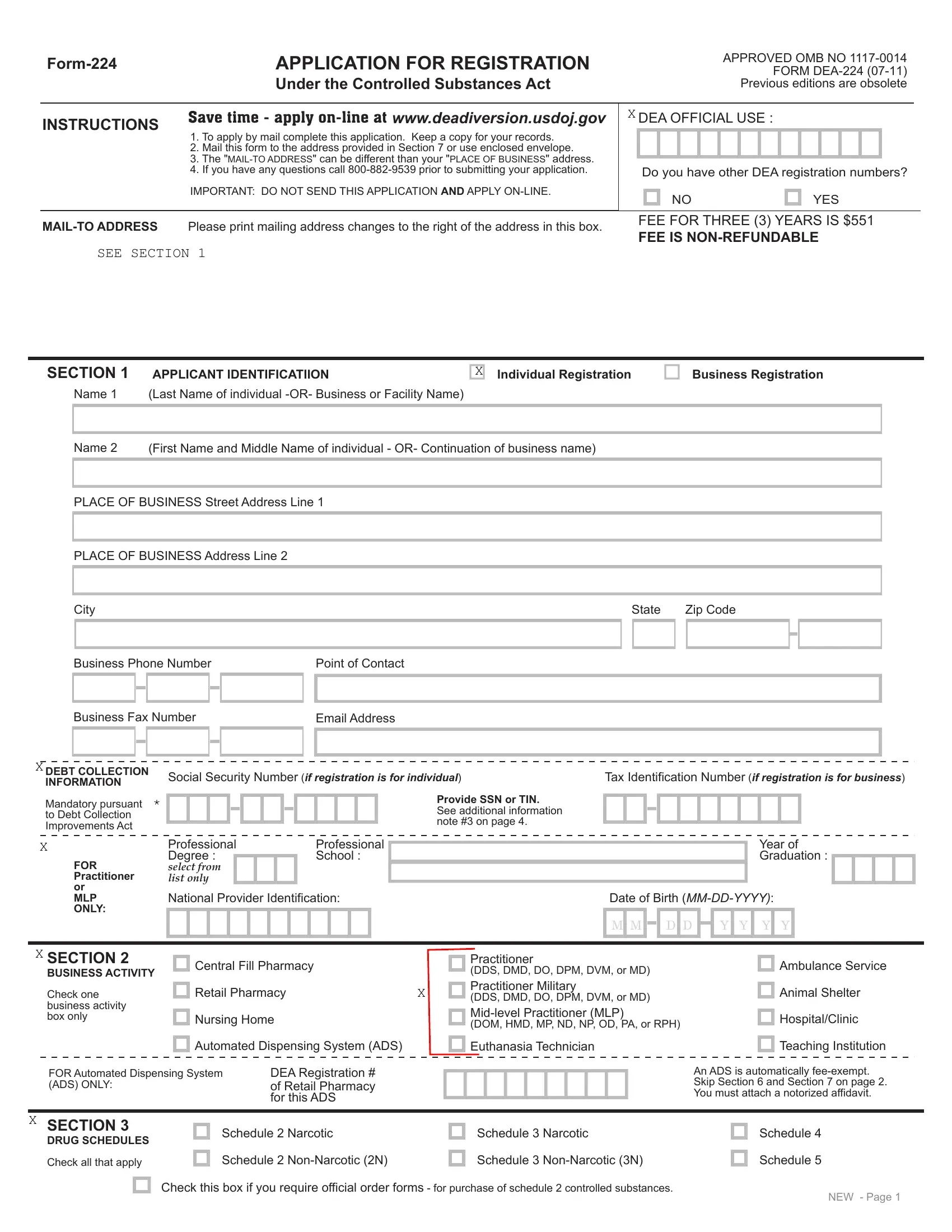
1. It is recommended to fill out the form 224 correctly, therefore be attentive while filling out the parts including these particular blank fields:
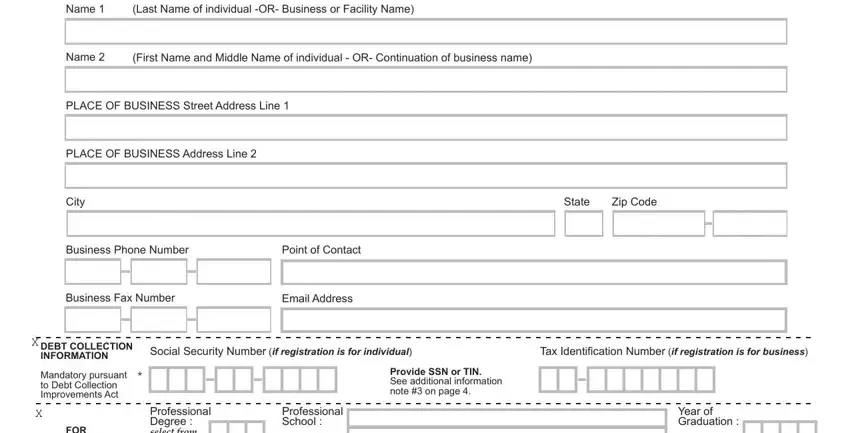
2. The subsequent step is usually to submit the next few blank fields: FOR Practitioner or MLP ONLY, SECTION BUSINESS ACTIVITY Check, National Provider Identification, Date of Birth MMDDYYYY, M M D D Y Y Y Y, Central Fill Pharmacy, Retail Pharmacy, Nursing Home, Practitioner DDS DMD DO DPM DVM or, Ambulance Service, Animal Shelter, HospitalClinic, Automated Dispensing System ADS, Euthanasia Technician, and Teaching Institution.
3. This part is going to be hassle-free - fill out all the empty fields in STATE LICENSE, MANDATORY, State License Number, What state was this license issued, SECTION, Expiration Date Has the applicant, MM DD YYYY, LIABILITY action pending, IMPORTANT, All questions in this section must, Dates of incident MMDDYYYY, Has the applicant ever, Dates of incident MMDDYYYY, Has the applicant ever, and Dates of incident MMDDYYYY in order to complete this segment.
4. This fourth part arrives with the following blanks to enter your details in: Applicants who have answered YES, Nature of incident, Disposition of incident, SECTION X, EXEMPTION FROM APPLICATION FEE, Check this box if the applicant is, Does not apply to, Business or Facility Name of Fee, FEE EXEMPT CERTIFIER, Provide the name and phone number, SECTION, METHOD OF PAYMENT, Check one form of payment only, The undersigned hereby certifies, and Signature of certifying official.
5. The document must be finalized with this particular part. Further there is a comprehensive listing of form fields that need specific details to allow your form usage to be accomplished: DEA Headquarter ATTN Registration, FEE IS NONREFUNDABLE, Sign if paying by credit card, Signature of Card Holder, Printed Name of Card Holder, SECTION, APPLICANTS SIGNATURE, Sign in ink, I certify that the foregoing, Signature of applicant sign in ink, Date, Print or type name and title of, and WARNING USC d states that any.
It is easy to make a mistake when filling out your DEA Headquarter ATTN Registration, thus make sure to reread it before you finalize the form.
Step 3: Spell-check all the details you've inserted in the blank fields and press the "Done" button. Grab your form 224 the instant you register at FormsPal for a free trial. Easily view the pdf form in your FormsPal account, with any edits and changes being conveniently saved! FormsPal offers protected document editor with no personal data recording or sharing. Rest assured that your data is safe here!