
SUFFIX can be completed effortlessly. Simply open FormsPal PDF tool to perform the job without delay. To have our editor on the leading edge of practicality, we aim to implement user-driven capabilities and enhancements regularly. We're always happy to receive feedback - join us in revolutionizing PDF editing. All it takes is a couple of simple steps:
Step 1: Open the form inside our editor by hitting the "Get Form Button" above on this page.
Step 2: This editor offers the ability to work with your PDF document in many different ways. Modify it with personalized text, adjust what is originally in the document, and place in a signature - all when it's needed!
This PDF form will need specific data to be filled in, thus make sure to take some time to type in what is expected:
1. You need to complete the SUFFIX accurately, so be careful when filling in the sections that contain all of these blank fields:
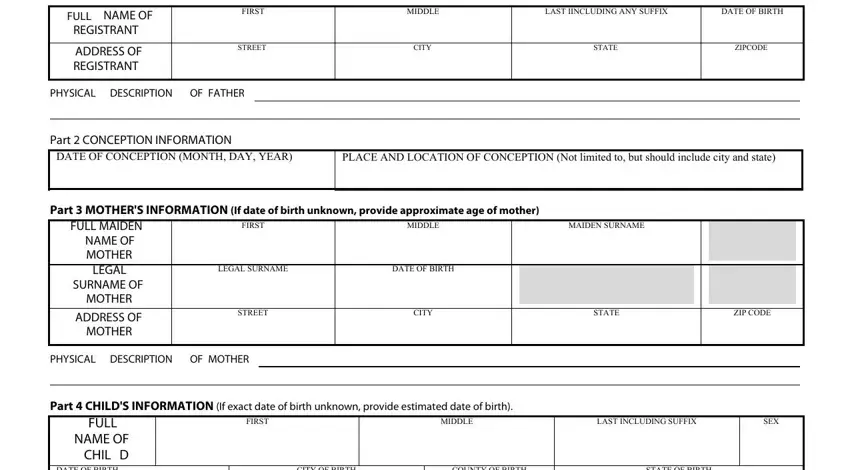
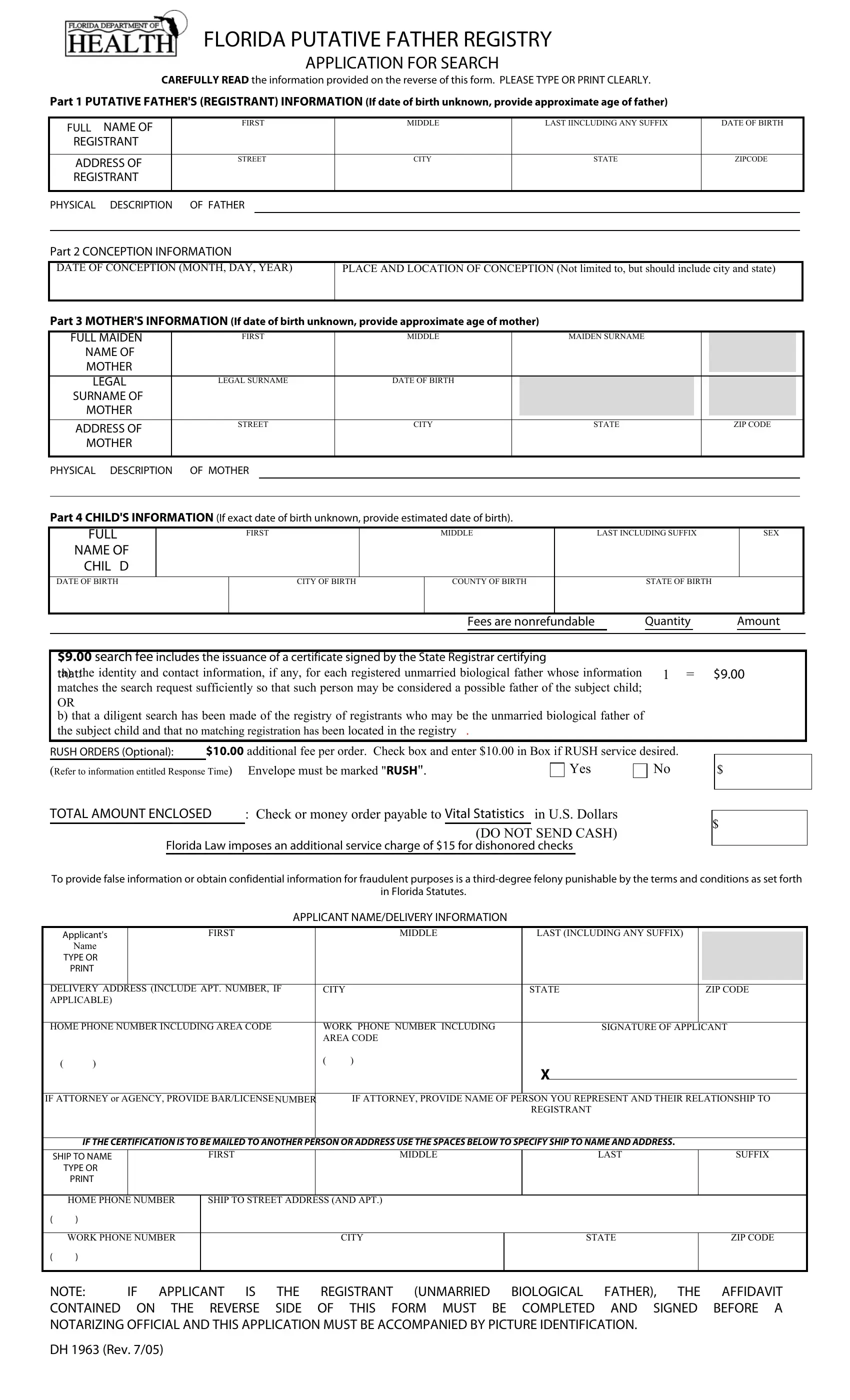
2. The next part would be to fill out the next few fields: DATE OF BIRTH, CITY OF BIRTH, COUNTY OF BIRTH, STATE OF BIRTH, Fees are nonrefundable, Quantity, Amount, search fee includes the issuance, RUSH ORDERS Optional Refer to, additional fee per order Check, Yes, TOTAL AMOUNT ENCLOSED, Check or money order payable to, Florida Law imposes an additional, and To provide false information or.
3. Completing DELIVERY ADDRESS INCLUDE APT, CITY, STATE, ZIP CODE, HOME PHONE NUMBER INCLUDING AREA, WORK PHONE NUMBER INCLUDING AREA, SIGNATURE OF APPLICANT, IF ATTORNEY or AGENCY PROVIDE, IF ATTORNEY PROVIDE NAME OF PERSON, REGISTRANT, IF THE CERTIFICATION IS TO BE, SHIP TO NAME, TYPE OR PRINT, FIRST, and MIDDLE is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Be very careful when completing MIDDLE and STATE, since this is the part in which a lot of people make mistakes.
Step 3: Check all the information you've typed into the blank fields and then click on the "Done" button. Right after setting up a7-day free trial account here, you'll be able to download SUFFIX or send it via email right off. The PDF file will also be readily accessible through your personal cabinet with your modifications. At FormsPal, we strive to be sure that all your details are maintained secure.