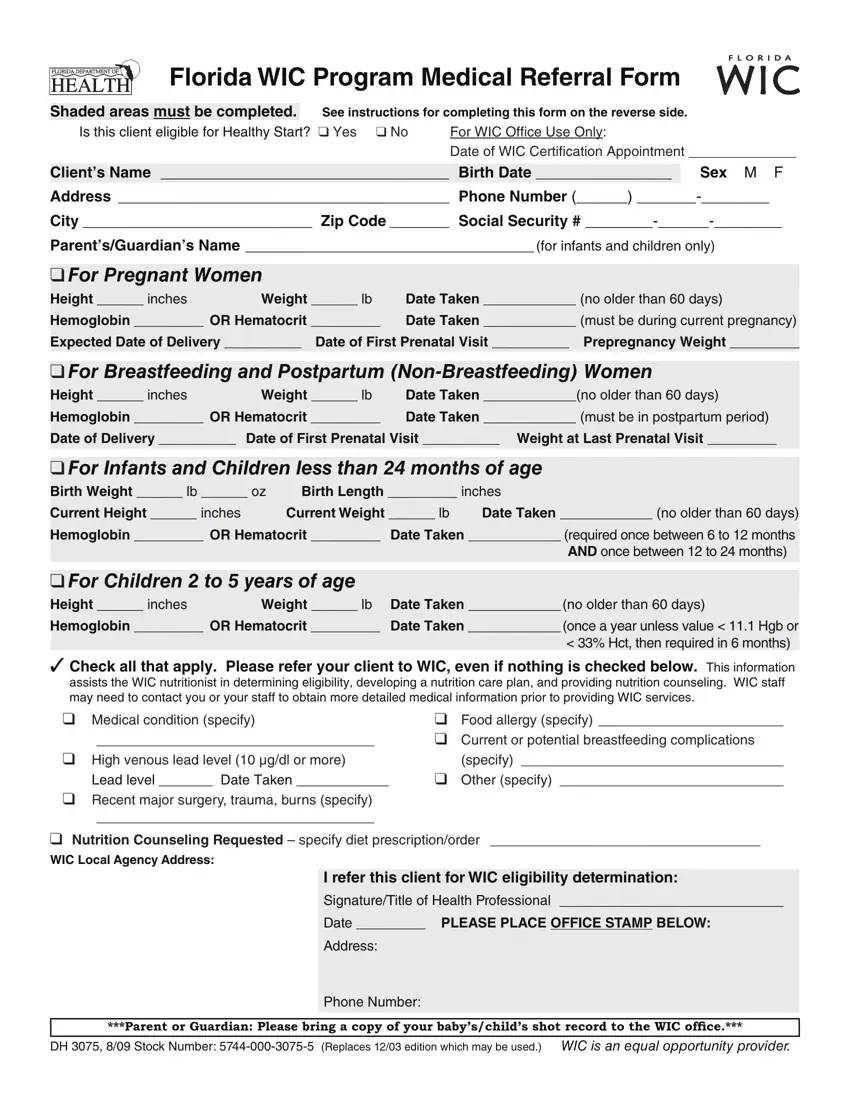
Florida WIC Program Medical Referral Form
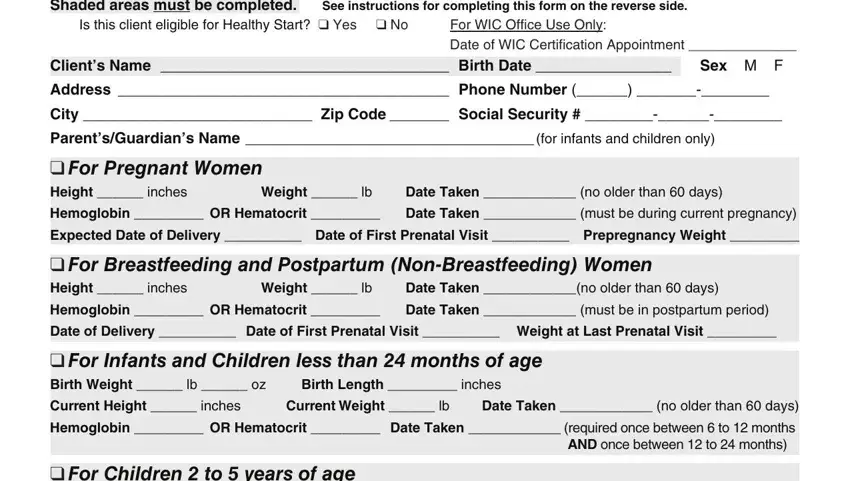
Shaded areas must be completed. See instructions for completing this form on the reverse side.
Is this client eligible for Healthy Start? ❑ Yes ❑ No |
For WIC Office Use Only: |
|
|
Date of WIC Certification Appointment ______________ |
|
|
|
Client’s Name __________________________________ |
Birth Date ________________ |
Sex M F |
Address _______________________________________ |
Phone Number (______) _______-________ |
City ___________________________ Zip Code _______ |
Social Security # ________-______-________ |
Parent’s/Guardian’s Name __________________________________ (for infants and children only)
❑ For Pregnant Women
Height ______ inches |
Weight ______ lb |
Date Taken ____________ (no older than 60 days) |
Hemoglobin _________ OR Hematocrit _________ |
Date Taken ____________ (must be during current pregnancy) |
Expected Date of Delivery __________ Date of First Prenatal Visit __________ Prepregnancy Weight _________
❑For Breastfeeding and Postpartum (Non-Breastfeeding) Women
Height ______ inches |
Weight ______ lb |
Date Taken ____________(no older than 60 days) |
Hemoglobin _________ OR Hematocrit _________ |
Date Taken ____________ (must be in postpartum period) |
Date of Delivery __________ |
Date of First Prenatal Visit __________ Weight at Last Prenatal Visit _________ |
❑For Infants and Children less than 24 months of age
Birth Weight ______ lb ______ oz |
Birth Length _________ inches |
Current Height ______ inches |
Current Weight ______ lb |
Date Taken ____________ (no older than 60 days) |
Hemoglobin _________ OR Hematocrit _________ Date Taken ____________ (required once between 6 to 12 months
AND once between 12 to 24 months)
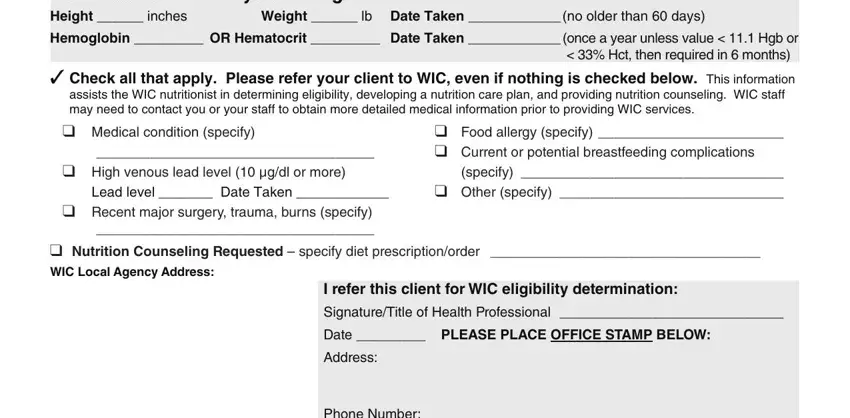
❑For Children 2 to 5 years of age
Height ______ inches |
Weight ______ lb |
Date Taken ____________ (no older than 60 days) |
Hemoglobin _________ OR Hematocrit _________ |
Date Taken ____________ (once a year unless value < 11.1 Hgb or |
|
|
< 33% Hct, then required in 6 months) |
✓Check all that apply. Please refer your client to WIC, even if nothing is checked below. This information
assists the WIC nutritionist in determining eligibility, developing a nutrition care plan, and providing nutrition counseling. WIC staff may need to contact you or your staff to obtain more detailed medical information prior to providing WIC services.
❑Medical condition (specify)
____________________________________
❑High venous lead level (10 μg/dl or more)
Lead level _______ Date Taken ____________
❑Recent major surgery, trauma, burns (specify)
____________________________________
❑Food allergy (specify) ________________________
❑Current or potential breastfeeding complications (specify) __________________________________
❑Other (specify) _____________________________
❑Nutrition Counseling Requested – specify diet prescription/order ___________________________________
WIC Local Agency Address:
I refer this client for WIC eligibility determination:
Signature/Title of Health Professional _____________________________
Date _________ PLEASE PLACE OFFICE STAMP BELOW:
Address:
Phone Number:
***Parent or Guardian: Please bring a copy of your baby’s/child’s shot record to the WIC ofice.***
DH 3075, 8/09 Stock Number: 5744-000-3075-5 (Replaces 12/03 edition which may be used.) WIC is an equal opportunity provider.
Instructions for Completing the Florida WIC Program Medical Referral Form
All shaded areas must be completed in order for the form to be processed.
1.Check (✓) YES if the client has been screened and is eligible for Healthy Start. Check (✓) NO if the client is not eligible for Healthy Start. Leave blank if the client has not been screened. Note: Eligibility for Healthy Start does not affect a client’s eligibility for WIC.
2.Complete the client’s name and birth date.
3.Optional Information: the client’s sex, mailing address, phone number, city, zip code, social security number, and the parent’s or guardian’s name for infants and children.
4.Complete the appropriate shaded section for the client.
Pregnant Women: Complete the height and weight measurements and the date they were taken. These measurements are to be taken no more than 60 days before the client’s WIC appointment. (The WIC appointment may be recorded at the top of the form.) Complete the hemoglobin or hematocrit value and the date the value was taken. There is no limit on how old the bloodwork data can be, as long as the measurement was taken during the current pregnancy. Complete the expected date of delivery, the date of the client’s first prenatal visit, and the prepregnancy weight.
Breastfeeding Women (eligible up to one year after delivery) and Postpartum Women—Non-Breastfeeding (eligible up to 6 months after delivery/termination of pregnancy): Complete the height and weight measurements and the date they were taken. These measurements are to be taken no more than 60 days before the client’s WIC appointment. (The WIC appointment may be recorded at the top of the form.) Complete the hemoglobin or hematocrit value and the date the value was taken. There is no limit on how old the bloodwork data can be, as long as the bloodwork is taken after delivery of the most recent pregnancy. Complete the actual date of delivery, the date of the first prenatal visit, and the weight measurement at the last prenatal visit.
Infants and Children less than 24 months of age: Complete the infant’s birth weight and birth length. Complete the current height and weight measurements and the date they were taken. These measurements are to be taken no more than 60 days before the client’s WIC appointment. (The WIC appointment may be recorded at the top of the form.) Complete the hemoglobin or hematocrit value and the date the value was taken. A bloodwork value is required once during infancy between 6 to 12 months of age (preferably between 9 to 12 months of age) and once between 1 to 2 years of age (preferably 6 months from the infant bloodwork value).
Children 2 to 5 years of age: Complete the current height and weight measurements and the date they were taken. These measurements are to be taken no more than 60 days before the client’s WIC appointment. (The WIC appointment may be recorded at the top of the form.) Complete the hemoglobin or hematocrit value and the date the value was taken. A bloodwork value is required once a year unless the value is abnormal
(< 11.1 hemoglobin or < 33% hematocrit), then a bloodwork value is required in 6 months.
5.Check (✓) any health problem that you have identified. Even if you have not identified a health problem, refer the client to the WIC program.
6.If you would like a nutritionist to counsel your client on a specific diet, check the box and specify the diet prescription or diet order requested.
7.If possible, please provide a copy of the immunization record for infant and child clients.
8.Complete the shaded area at the bottom of the form with the signature of the health professional taking the measurement or his/her designee and the office address and phone number. Stamp the form with the office stamp or the health professional’s stamp.
9.Give this completed form to the client or parent/guardian to bring to the WIC certification appointment or mail/fax the form to the local WIC agency address shown in the bottom left corner of the form.