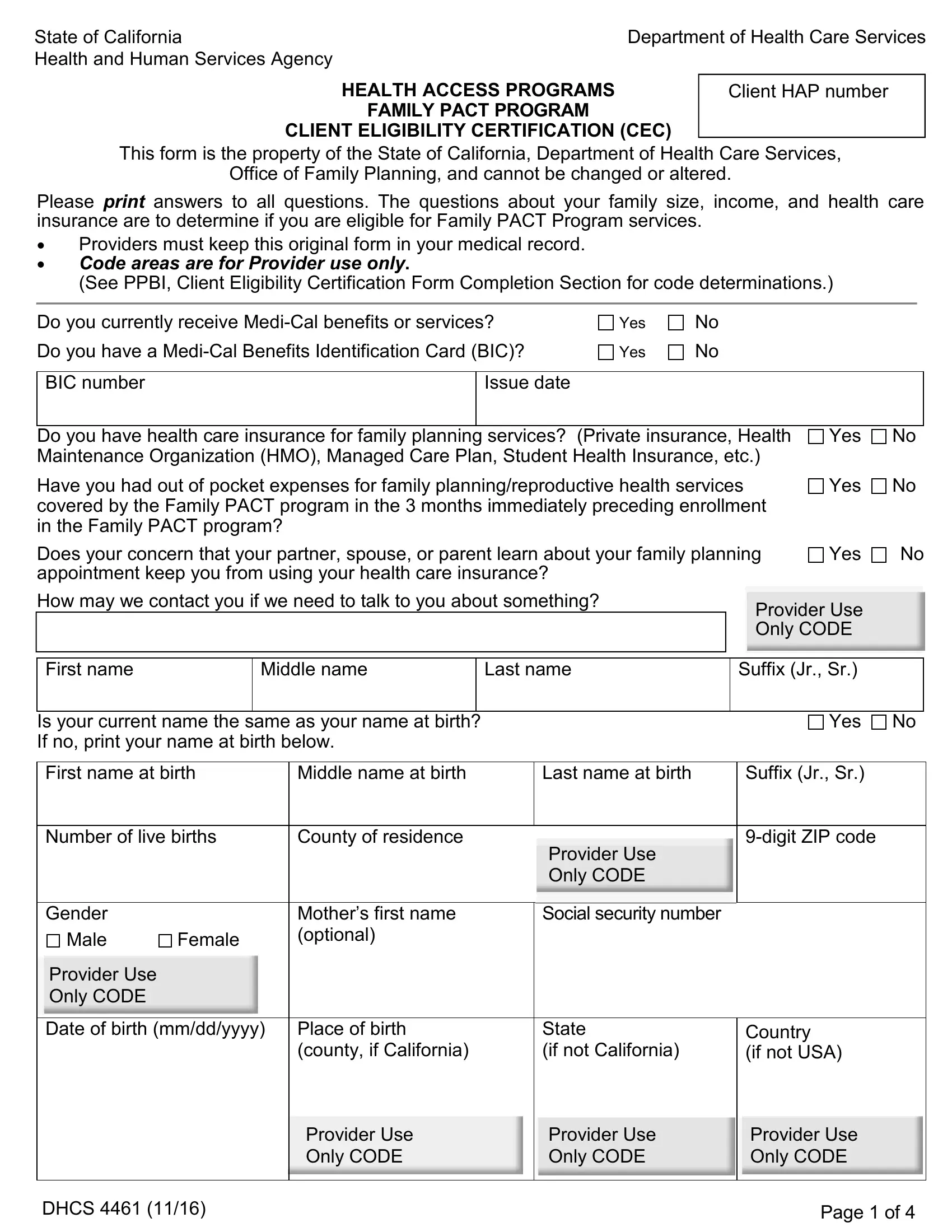
The DHCS 4461 form, a pivotal document issued by the State of California Department of Health Care Services, plays a critical role in the administration of the Family PACT Program. This form, standing as the gateway for clients to certify their eligibility, encompasses a series of questions focused on family size, income, and existing health care insurance to ascertain if applicants meet the criteria for the program's services. Notably, it underscores the program's commitment to privacy and the individual's right to confidential family planning services, addressing concerns such as the fear of insurance use disclosure to partners, parents, or spouses. It also includes provisions for those who have incurred out-of-pocket expenses for family planning and reproductive health services in the recent past, setting the stage for potential reimbursement or coverage under the program. With sections dedicated to both applicant and provider use, including eligibility determination and provider certification, the form is designed to ensure a thorough and confidential evaluation process. Furthermore, it highlights the importance of accuracy and honesty in the application process, warning of the repercussions of falsifying information. Alongside these features, the form extends an array of linguistic support services, ensuring that non-English speakers have full access to the program's benefits, thereby embodying the inclusivity and accessibility at the core of health access programs in California.
| Question | Answer |
|---|---|
| Form Name | Form Dhcs 4461 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | dhcs 4461 form, client eligibility, dhcs 4461, california dhcs health access pact |
State of California |
Department of Health Care Services |
Health and Human Services Agency |
|
HEALTH ACCESS PROGRAMS
FAMILY PACT PROGRAM
CLIENT ELIGIBILITY CERTIFICATION (CEC)
Client HAP number
This form is the property of the State of California, Department of Health Care Services,
Office of Family Planning, and cannot be changed or altered.
Please print answers to all questions. The questions about your family size, income, and health care insurance are to determine if you are eligible for Family PACT Program services.
•Providers must keep this original form in your medical record.
•Code areas are for Provider use only.
(See PPBI, Client Eligibility Certification Form Completion Section for code determinations.)
Do you currently receive
Do you have a
Yes No
Yes No
BIC number
Issue date
Do you have health care insurance for family planning services? (Private insurance, Health |
Yes |
No |
||
Maintenance Organization (HMO), Managed Care Plan, Student Health Insurance, etc.) |
|
|
||
Have you had out of pocket expenses for family planning/reproductive health services |
|
Yes |
No |
|
covered by the Family PACT program in the 3 months immediately preceding enrollment |
|
|
||
in the Family PACT program? |
|
|
|
|
Does your concern that your partner, spouse, or parent learn about your family planning |
Yes |
No |
||
appointment keep you from using your health care insurance? |
|
|
|
|
How may we contact you if we need to talk to you about something? |
|
|
|
|
Provider Use |
|
|||
|
|
|
||
|
|
Only CODE |
|
|
|
|
|
|
|
First name
Middle name
Last name
Suffix (Jr., Sr.)
Is your current name the same as your name at birth? |
|
|
Yes No |
||||
If no, print your name at birth below. |
|
|
|
|
|||
|
|
|
|
|
|
||
First name at birth |
Middle name at birth |
Last name at birth |
|
Suffix (Jr., Sr.) |
|||
|
|
|
|
|
|
||
Number of live births |
County of residence |
|
|
||||
|
|
|
|
Provider Use |
|
|
|
|
|
|
|
Only CODE |
|
|
|
|
|
|
|
|
|
|
|
Gender |
|
|
Mother’s first name |
Social security number |
|
|
|
Male |
Female |
(optional) |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Provider Use |
|
|
|
|
|
|
|
Only CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Date of birth (mm/dd/yyyy) |
Place of birth |
State |
|
Country |
|||
|
|
|
(county, if California) |
(if not California) |
|
(if not USA) |
|
|
|
|
|
|
|
|
|
|
|
|
Provider Use |
Provider Use |
|
Provider Use |
|
|
|
|
Only CODE |
Only CODE |
|
Only CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DHCS 4461 (11/16) |
Page 1 of 4 |
Race/ethnicity
1 Asian
5 Native American
Primary Language
3 |
English |
1 |
8 |
Spanish |
6 |
2 |
Black |
|
3 |
Filipino |
4 |
6 |
Pacific Islander |
7 |
White |
0 |
|
Armenian |
2 |
Cantonese |
4 |
Hmong |
5 |
Korean |
7 |
Tagalog |
9 |
Vietnamese |
0 |
Hispanic
Other
Khmer/Cambodian Other
Eligibility Determination: Please list all family members (self, spouse, and children) and all taxable income sources. If someone else claims you on their taxes, list everyone claimed and all related taxable income sources. Reportable income includes but is not limited to: income from employment,
Name |
Relationship |
Age |
Source of Income |
Taxable Monthly |
|
to You |
|
|
Income |
|
|
|
|
|
|
|
|
|
|
|
(Self) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Family size:
Total taxable family income $
I received information on how to apply for insurance affordability programs
Yes
No
I understand that I can visit CoveredCA.com or call
I declare under penalty of perjury under the laws of the state of California that the foregoing information on this form is true and correct. I understand that the giving of false information may make me ineligible for this program.
Signature (or mark) of applicant |
Signature of witness |
Date
Date
Privacy Statement (Civil Code § 1798 et seq.)
This information will be used to see if you are enrolled in any state health program. Information will also be used to monitor health outcomes and for program evaluation purposes. Your name will not be shared. Each individual has the right to review personal information maintained by the provider unless exempt under Article 8 of the Information Practices Act.
DHCS 4461 (11/16) |
Page 2 of 4 |

Provider certification:
FOR PROVIDER USE ONLY
Eligible for Family PACT Program
Ineligible for Family PACT Program (Give Fair Hearing Rights)
Why:
Limited scope
Unmet
Based upon the information provided by the applicant and according to state and federal requirements, I certify that the applicant identified on this Client Eligibility Certification is eligible to receive family planning services under the Family PACT Program. If ineligible, the client has received a copy of this form which includes the Fair Hearing Rights. I also certify that the client has received the Notice of Privacy Practices.
|
Print name |
Signature |
Date |
|
|
|
|
|
Deactivation: If client is deactivated |
Date |
Reason code |
|
(no longer eligible) |
|
(see Provider |
|
|
|
Manual) |
|
|
|
|
|
|
|
|
Fair Hearing Rights
Any applicant for, or recipient of, services under the Family PACT Program shall have a right to a hearing regarding eligibility or receipt of services. An applicant or recipient does not have a right to contest changes made to the eligibility standards or benefits of the Family PACT Program.
First level review: If you wish to appeal either your denial of eligibility or receipt of services, please send your name, telephone number, address, and reason why you are requesting a First Level Review to the address below. A request for a first level review must be postmarked within 20 working days of the denial of eligibility or services. The Office of Family Planning may request additional information by telephone or in writing from the provider or the applicant before issuing a decision.
Formal Hearing: You may request a formal hearing within 90 days from the day you were notified that you were not eligible or the services you wanted will not be provided or have been discontinued. If you have good cause as to why you were not able to file for a hearing within the 90 days, you may still file for a hearing. If you provide good cause, your request may still be scheduled. Provide all requested information such as your full name, telephone number, address, and the reason for the Formal Hearing and mail it to the Formal Hearing address below. If you wish, you may attach a letter as well and explain why you believe the action taken is not correct. You may also call the Public Inquiry and Response number below. If you have trouble understanding English, be sure to state your language so arrangements can be made to have language assistance at the hearing. If you have chosen an authorized representative, be sure to state his/her name, phone number and address. Keep a copy of your hearing request for your records. You may submit your formal hearing request in one of two ways:
First Level Review |
Formal Hearing |
or |
Department of Health Care Services |
California Department of |
Department of Social Services |
Office of Family Planning |
Social Services |
State Hearings Division |
P.O. Box 997413, Mail Station 8400 |
State Hearings Division |
Public Inquiry and Response |
Sacramento, CA |
P.O. Box 944243, |
|
|
Mail Station |
|
|
Sacramento, CA |
TDD |
|
|
Fax: (916) |
DHCS 4461 (11/16) |
Page 3 of 4 |
State of California |
Department of Health Care Services |
Health and Human Services Agency |
|
Language Services Notice
ﻢﻗر)
注意:如果您使用繁體中文,您可以免費獲得語言援助服務。請致電
TTY:711 [Chinese]
्यान द: यद आप हद� बोलतेह तो आपकेि◌लए म्तु म भाषा सहायता सेवाएंउपल्ध ह। 1-
LUS CEEV: Yog tias koj hais lus Hmoob, cov kev pab txog lus, muaj kev pab dawb rau
koj. Hu rau
주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다.
រ◌បយ័ត៖ េ◌េបើសិនអកនិយ ែ◌ខរ, េ◌សជំនួែយផក េ◌យមិនគិតឈល គឺចនសំប់បំេ◌រអក។ ចូរទរស័ពូ
ਿ◌ਧਆਨ ਿ◌ਦਓ: ਜੇਤੁਸ ਪੰ ਜਾਬੀਬੋਲਦੇਹੋ, ਤ ਭਾਸ਼ਾ ਿ◌ਵੱ ਚਸਹਾਇਤਾ ਸੇਵਾਤੁਹਾਡੇਲਈ ਮੁਫਤਉਪਲਬਧ ਹੈ। 1-
ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатные
услуги перевода. Звоните
PAUNAWA: Kung nagsasalita ka ng Tagalog, maaari kang gumamit ng mga serbisyo ng
tulong sa wika nang walang bayad. Tumawag sa
เรียน: ถาค้ ุณพดู ภาษาไทยคุณสามารถใชบ้ รกิ ารช่วยเหลอื ทางภาษาไดฟีโทร
CHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ miễn phí dành cho bạn.
Gọi số
DHCS 4461 (11/16) |
Page 4 of 4 |