Do you need to complete and submit a Form DHCS 4502 for Medi-Cal services? This form is used as part of the process when applying or renewing eligibility for certain community-based care programs. It helps verify household income and resources, so it’s important that applicants answer all questions accurately. With this blog post, we want to walk readers through the whole process of filling out the Form DHCS 4502 and what they can expect upon submitting it. Read on for more details about Medi-Cal services, how to fill out a Form DHCS 4502 correctly, and any other tips that could come in handy throughout the application requirements!
| Question | Answer |
|---|---|
| Form Name | Form Dhcs 4502 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | ITIN, medical application, disenrollment, E-mail |
State of |
Department of Health Care Services |
|
Children’s Medical Services Branch |
|
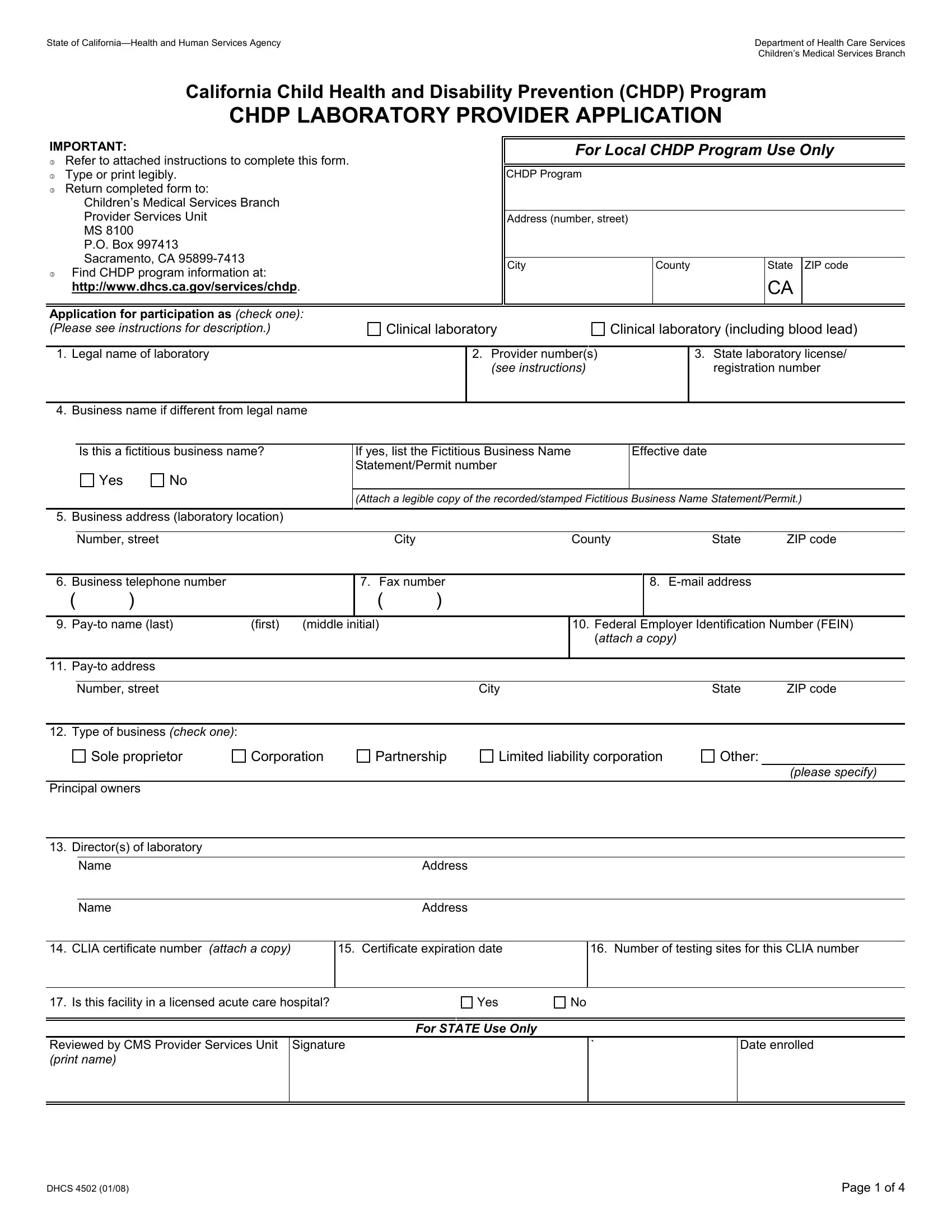
California Child Health and Disability Prevention (CHDP) Program |
||
|
CHDP LABORATORY PROVIDER APPLICATION |
||
IMPORTANT: |
|
|
|
|
|
|
|
|
|
For Local CHDP Program Use Only |
|
3Refer to attached instructions to complete this form.
3 |
Type or print legibly. |
|
|
CHDP Program |
|
|
|
|
|
|
3 |
Return completed form to: |
|
|
|
|
|
|
|
|
|
|
Children’s Medical Services Branch |
|
|
|
|
|
|
|
|
|
|
Provider Services Unit |
|
|
Address (number, street) |
|
|
|
|||
|
MS 8100 |
|
|
|
|
|
|
|
|
|
|
P.O. Box 997413 |
|
|
|
|
|
|
|
|
|
|
Sacramento, CA |
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
County |
|
State |
ZIP code |
||
|
Find CHDP program information at: |
|
|
|
|
|||||
3 |
|
|
|
|
|
|
|
|
|
|
|
http://www.dhcs.ca.gov/services/chdp. |
|
|
|
|
|
|
|
CA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Application for participation as (check one): |
|
|
|
|
|
|
|
|
|
|
(Please see instructions for description.) |
Clinical laboratory |
Clinical laboratory (including blood lead) |
||||||||
|
|
|
|
|
|
|
||||
|
1. Legal name of laboratory |
|
2. Provider number(s) |
|
|
3. |
State laboratory license/ |
|||
|
|
|
(see instructions) |
|
|
|
registration number |
|||
|
|
|
|
|
|
|
|
|
|
|
4. Business name if different from legal name
Is this a fictitious business name?
Yes |
No |
If yes, list the Fictitious Business Name |
Effective date |
Statement/Permit number |
|
|
|
(Attach a legible copy of the recorded/stamped Fictitious Business Name Statement/Permit.)
5. Business address (laboratory location)
Number, street |
City |
County |
State |
ZIP code |
6. Business telephone number
()
7. Fax number
()
8.
9. |
(first) (middle initial) |
10.Federal Employer Identification Number (FEIN) (attach a copy)
11.
Number, street |
City |
State |
ZIP code |
12. Type of business (check one):
Sole proprietor
Corporation
Partnership
Limited liability corporation
Other:
|
|
|
|
|
(please specify) |
Principal owners |
|
|
|
||
|
|
|
|
|
|
13. |
Director(s) of laboratory |
|
|
|
|
|
|
|
|
|
|
|
|
Name |
Address |
|
|
|
|
|
|
|
|
|
|
Name |
Address |
|
|
|
|
|
|
|
|
14. |
CLIA certificate number (attach a copy) |
15. Certificate expiration date |
|
16. Number of testing sites for this CLIA number |
|
|
|
|
|
|
|
17. |
Is this facility in a licensed acute care hospital? |
Yes |
No |
||
For STATE Use Only
Reviewed by CMS Provider Services Unit |
Signature |
` |
Date enrolled |
(print name) |
|
|
|
|
|
|
|
|
|
|
|
DHCS 4502 (01/08) |
Page 1 of 4 |
State of |
Department of Health Care Services |
|
Children’s Medical Services Branch |
The laboratory applicant hereby agrees to abide by the statutory and regulatory requirements and policies of the CHDP Program. The information submitted on this application and any attachments are true, accurate, and complete to the best of the Laboratory Applicant’s knowledge and belief and are furnished in good faith. The Laboratory Applicant understands that failure to comply with the requirements of the CHDP Program may result in disenrollment.
18. Printed name of Laboratory Director (first) |
(middle initial) |
(last) |
19. Laboratory Director signature IN BLUE INK ONLY
Date
20. Printed name of Owner (first) |
(middle initial) |
(last) |
21. Owner signature IN BLUE INK ONLY
Date
Privacy Statement (as required by Civil Code, Section 1798 et seq.)
All information requested on the application is required by the Department of Health Care Services (DHCS) by the authority of Title 17, Section 6860. The consequences of not supplying the requested information are denial of enrollment as a CHDP provider and no issuance of the provider number to obtain reimbursement from the CHDP Program. Any information provided will be used to verify eligibility to participate as a provider in the CHDP Program. Any information may also be provided to the State Controller’s Office, the California Department of Justice, the Department of Consumer Affairs, the Department of Corporations, or other state or local agencies as appropriate, fiscal intermediaries, managed care plans, the Federal Bureau of Investigation, the Internal Revenue Service, Medicare fiscal intermediaries, Centers for Medicare and Medicaid Services, Office of the Inspector General, and Medicaid and licensing programs in other states. For more information or access to records containing your personal information maintained by DHCS, contact the Provider Services Unit of Children’s Medical Services Branch, MS 8100, P.O. Box 997413, Sacramento, CA
DHCS 4502 (01/08) |
Page 2 of 4 |
State of |
Department of Health Care Services |
|
Children’s Medical Services Branch |
INSTRUCTIONS FOR COMPLETION OF THE
CHDP LABORATORY PROVIDER APPLICATION
For assistance in completing this application, please call the CMS Branch,
Provider Services Unit at (916)
Laboratory providers wishing to enroll as a provider with the CHDP Program must complete an application and be approved by the California Children’s Medical Services Branch in order to bill the CHDP Program for CHDP services.
Upon review and approval of the completed application, the applicant will be assigned a provider number to use when billing the CHDP Program. Omission of any information or documentation on this application or the failure to sign this application may result in delays in processing or inability to process this application. Applicants may be contacted orally or in writing if additional information and documentation are needed.
Application for participation as: Mark the appropriate box indicating the type of laboratory for which you are applying.
A clinical laboratory must be:
3Licensed or registered by the Department pursuant to the Business and Professions Code, Section 1265; and
3Hold the appropriate certification or approval under CLIA for the level of testing done in the laboratory.
A clinical laboratory (including blood lead) must be:
3Licensed or registered by the Department pursuant to the Business and Professions Code, Section 1265;
3Certified or approved under CLIA for nonwaived testing and for subspecialty toxicology, analyte blood lead; and
3Enrolled in, and qualified as proficient in blood lead level analysis by, the California Blood Lead Proficiency Assurance Program administered by Department, refer to http://www.dhs.ca.gov/ehlb/BioChem or (510)
1.Legal name of laboratory means the name under which the applicant is applying for a CHDP provider number and listed with the IRS.
2.Provider number(s): Provide all active provider numbers of the applicant. Provide only the active provider numbers that are assigned to the business address indicated on this form.
3.State laboratory license/registration number: Provide the registration number and a legible copy of the license/registration.
4.Business name means the name of the laboratory applicant if different from that listed in number 1. If this is a fictitious business name, provide the Fictitious Business Name Statement/Permit number and effective date. Attach a legible copy of the recorded/stamped Fictitious Business Name Statement/Permit to the application.
5.Business address (location/site of laboratory) means the location where the applicant is providing services, including the street name and number, room or suite number or letter, city, county, state, and
6.Business telephone number means the primary business telephone number used at the applicant’s business address. A beeper number, answering service, answering machine, pager, facsimile machine, or cellular phone is not acceptable as the business telephone number.
7.Fax number means the facsimile number used at the business address.
8.
9.
10.Enter the Federal Employer Identification Number (FEIN) issued by the IRS under the name of the Laboratory Applicant. Attach a legible copy of the IRS Form 941, Form
11.The
12.Indicate the type of business that applies to your business structure. Provide the names of the principal owners.
13.Enter the name(s) of the director(s) of the laboratory and the address where contact can be made.
DHCS 4502 (01/08) |
Page 3 of 4 |

State of |
Department of Health Care Services |
|
Children’s Medical Services Branch |
14.Provide the current CLIA certificate number and attach a legible copy of the certificate to the application.
15.Enter the expiration date of the CLIA certificate.
16.Enter the number of testing sites to which the CLIA certificate applies.
17.Mark the appropriate box indicating whether or not this lab is located in a licensed acute care hospital.
18.Print the first name, middle initial, and last name of the Laboratory Director.
19.Laboratory Director signature means the first name, middle name, and last name of the Laboratory Director. An original signature IN BLUE INK ONLY is required. Indicate the date the application is signed. NOTE: Laboratory Director signature on the CHDP Laboratory Provider Program Agreement (DHCS 4503) means the name and signature of the Laboratory Director indicated in number 19.
20.Print the first name, middle initial, and last name of the Laboratory Owner.
21.Laboratory Owner signature means the first name, middle initial, and last name of the Laboratory Owner. An original signature IN BLUE INK ONLY is required. Indicate the date the application is signed. NOTE: Laboratory Owner signature on the CHDP Laboratory Provider Program Agreement (DHCS 4503) means the name and signature of the Laboratory Owner indicated in number 21.
Did you remember to enclose (as applicable):
The original, signed CHDP Laboratory Provider Program Agreement (DHCS 4503)
Copy of FEIN or ITIN verification or social security card, if applicable
Copy of Fictitious Business Name Statement/Permit, if applicable
Copy of CLIA certificate
Copy of laboratory license/registration
Other, if applicable
Send completed form to: |
Children’s Medical Services Branch |
|
Provider Services Unit |
|
MS 8100 |
|
P.O. Box 997413 |
|
Sacramento, CA |
DHCS 4502 (01/08) |
Page 4 of 4 |