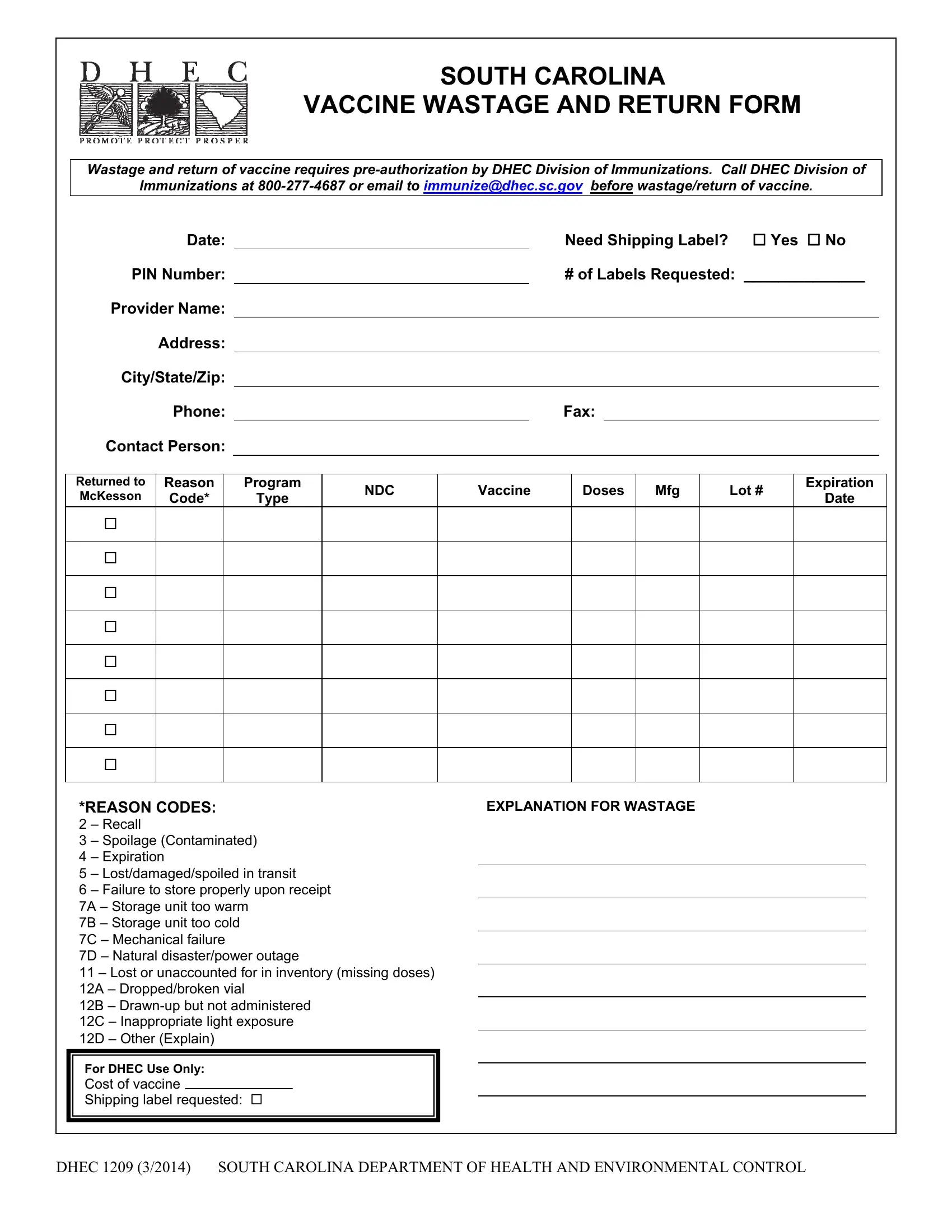
In the realm of vaccine management, the South Carolina Vaccine Wastage and Return Form, known as the DHEC 1209 form, plays a crucial role in ensuring vaccines' effective distribution and utilization. Crafted by the South Carolina Department of Health and Environmental Control (DHEC), this document is designed for meticulous record-keeping of any vaccines that are either wasted or need to be returned. The form requires pre-authorization from the DHEC’s Division of Immunizations, a step that underlines the importance of accountability before any vaccine-related action is taken. It outlines clear instructions for providers, including the need for detailed information about the vaccines in question—such as the reason for wastage or return, type of program (VFC or State), National Drug Code (NDC), and specific details about the vaccine manufacturer, lot number, and expiration date. Additionally, the form delves into logistics, such as whether a shipping label is needed for the return of vaccines to McKesson, the CDC's central distributor. Providers are guided to furnish a written explanation for the wastage, an action that reinforces the form's role in promoting transparency and enabling better vaccine management practices. With spaces dedicated to explaining the specific reasons for wastage—ranging from recalls to spoilage, and even natural disasters—this form encapsulates the multifaceted nature of vaccine stewardship, highlighting the meticulous care and detailed planning that go into ensuring vaccine efficacy and safety.
| Question | Answer |
|---|---|
| Form Name | Form Dhec 1209 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | D 1209 dhec expiration form |
SOUTH CAROLINA
VACCINE WASTAGE AND RETURN FORM
Wastage and return of vaccine requires
Immunizations at
|
Date: |
|
|
|
|
|
Need Shipping Label? |
Yes No |
|
||||||||
PIN Number: |
|
|
|
|
|
# of Labels Requested: ______________ |
|
||||||||||
Provider Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City/State/Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Phone: |
|
|
|
|
|
Fax: |
|
|
|
|
|
|
||||
Contact Person: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Returned to |
Reason |
|
Program |
NDC |
|
Vaccine |
|
Doses |
Mfg |
|
Lot # |
Expiration |
|
||||
McKesson |
Code* |
|
|
Type |
|
|
|
Date |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
*REASON CODES: |
|
|
|
EXPLANATION FOR WASTAGE |
|
|
|
|
|||||||||
2 – Recall |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 – Spoilage (Contaminated) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
4 – Expiration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
5 – Lost/damaged/spoiled in transit
6 – Failure to store properly upon receipt
7A – Storage unit too warm
7B – Storage unit too cold
7C – Mechanical failure
7D – Natural disaster/power outage
11 – Lost or unaccounted for in inventory (missing doses) 12A – Dropped/broken vial
12B –
12C – Inappropriate light exposure
12D – Other (Explain)
For DHEC Use Only:
Cost of vaccine
Shipping label requested:
DHEC 1209 (3/2014) SOUTH CAROLINA DEPARTMENT OF HEALTH AND ENVIRONMENTAL CONTROL
SOUTH CAROLINA DEPARTMENT OF HEALTH AND ENVIRONMENTAL CONTROL
South Carolina
Vaccine Wastage and Return Form
Instructions for Completing
Purpose:
The purpose of the Vaccine Wastage and Return Form is to record the wastage and/or return of vaccine.
Wastage/ Return of vaccine requires
1.Provider will enter identifying information about the provider’s office from which the vaccine is wasted/ returned. All information is required.
2.Provider will enter information for each vaccine being wasted/ returned including Reason Code, Program Type (for example VFC or State), NDC, Vaccine Name, Doses, Manufacturer (Mfg), Lot Number and Expiration Date.
3.If provider is directed by DHEC Immunization Division to return vaccine to McKesson (CDC’s Central Distributor) for excise tax, place a check in the “Returned to McKesson” column.
4.Provider will indicate if a shipping label is needed for return of the vaccine to McKesson and how many labels the provider is requesting. Vaccine is to be returned to McKesson within six months of the expiration date.
5.Provider must provide a written explanation for wastage in space provided.
Office Mechanics and Filing:
1.Provider must fax the completed form to DHEC Immunization Division
2.Form Retention:
3.If the provider is directed to return vaccine to McKesson, a copy of the completed form must be sent with the vaccine to McKesson.
DHEC 1209 (3/2014) SOUTH CAROLINA DEPARTMENT OF HEALTH AND ENVIRONMENTAL CONTROL