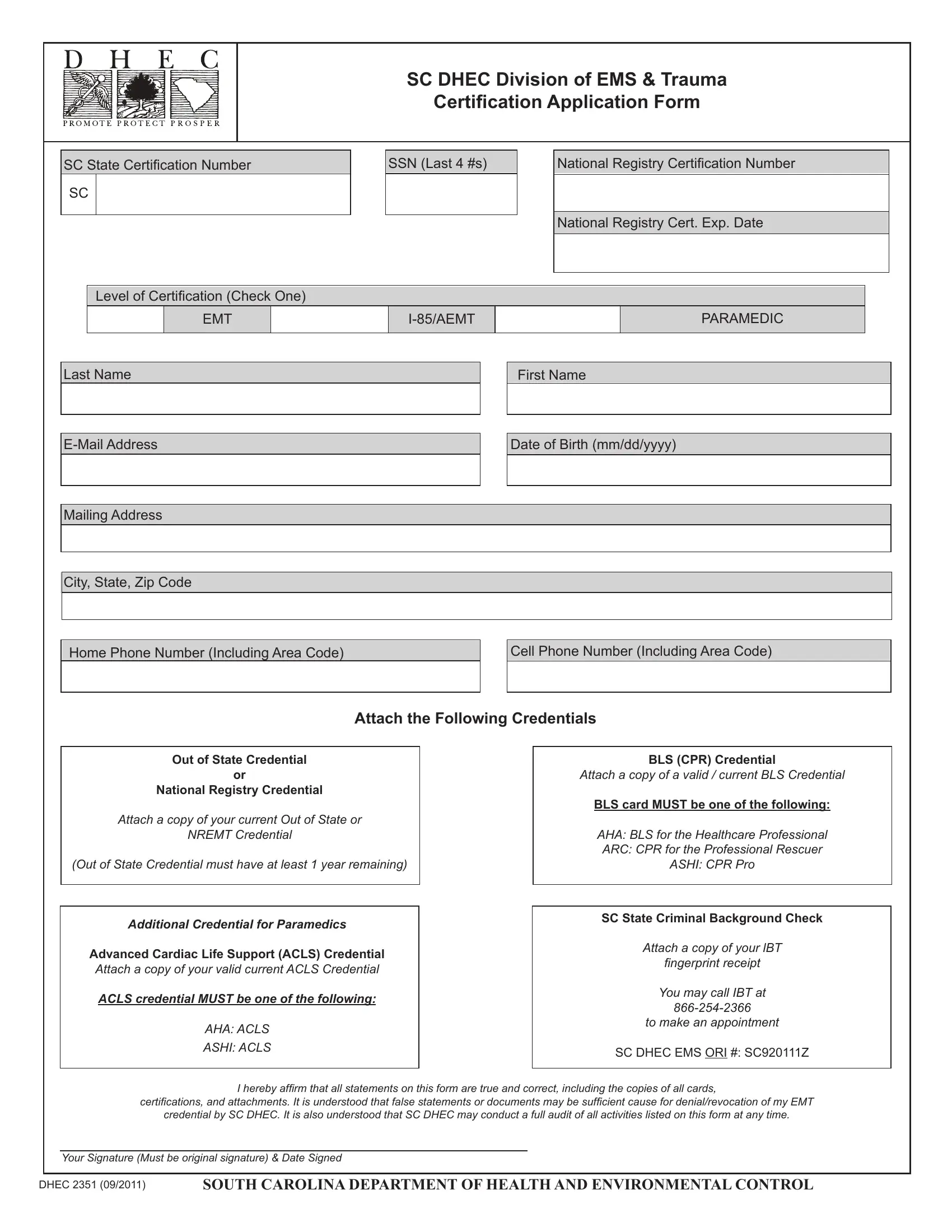
The DHEC 2351 form plays a crucial role in the certification and recertification process for Emergency Medical Technicians (EMTs) and Paramedics within South Carolina, acting under the jurisdiction of the South Carolina Department of Health and Environmental Control (SC DHEC) Division of EMS & Trauma. This form is integral for professionals either seeking initial certification or renewal in the state. It requires applicants to provide their South Carolina state certification number, the last four digits of their Social Security Number (SSN), National Registry Certification Number, and the expiration date of their national registration. Furthermore, it delineates the level of certification being applied for, ranging from EMT, Intermediate to Advanced EMT (AEMT), and Paramedic, demanding personal details along with contact information for thorough completion. The form mandates the attachment of specific credentials such as a valid out-of-state or National Registry Emergency Medical Technician (NREMT) credential, an Advanced Cardiac Life Support (ACLS) credential for paramedics, and a Basic Life Support (BLS) credential. Moreover, compliance with a South Carolina state criminal background check, evidenced by attaching a fingerprint receipt, is required. This juxtaposition of personal verification, professional qualification evidence, and legal clearance underscores the comprehensive approach South Carolina takes in ensuring that its emergency medical personnel are thoroughly vetted and qualified. By affirming the accuracy and authenticity of all statements and documents submitted, the applicant acknowledges the importance of integrity in the process, with the understanding that any falsification may lead to denial or revocation of certification. SC DHEC reserves the right to audit the submitted information, reinforcing the rigorous standards upheld in the certification process for emergency medical service providers in South Carolina.
| Question | Answer |
|---|---|
| Form Name | Form Dhec 2351 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dhec 2351, SSN, ASHI, EMT |
SC DHEC DIVISION OF EMS & TRAUMA
Certiication Application Form
SC State Certiication Number
SC
SSN (Last 4 #s)
National Registry Certiication Number
National Registry Cert. Exp. Date
Level of Certiication (Check One)
EMT
PARAMEDIC
Last Name
First Name
Date of Birth (mm/dd/yyyy)
Mailing Address
City, State, Zip Code
Home Phone Number (Including Area Code)
Cell Phone Number (Including Area Code)
Attach the Following Credentials
Out of State Credential
OR
National Registry Credential
Attach a copy of your current Out of State or
NREMT Credential
(Out of State Credential must have at least 1 year remaining)
Additional Credential for Paramedics
Advanced Cardiac Life Support (ACLS) Credential
Attach a copy of your valid current ACLS Credential
ACLS credential MUST be one of the following:
AHA: ACLS
ASHI: ACLS
BLS (CPR) Credential
Attach a copy of a valid / current BLS Credential
BLS card MUST be one of the following:
AHA: BLS for the Healthcare Professional ARC: CPR for the Professional Rescuer ASHI: CPR Pro
SC State Criminal Background Check
Attach a copy of your lBT
ingerprint receipt
You may call IBT at
to make an appointment
SC DHEC EMS ORI #: SC920111Z
I hereby afirm that all statements on this form are true and correct, including the copies of all cards,
certiications, and attachments. It is understood that false statements or documents may be suficient cause for denial/revocation of my EMT
credential by SC DHEC. It is also understood that SC DHEC may conduct a full audit of all activities listed on this form at any time.
Your Signature (Must be original signature) & Date Signed
DHEC 2351 (09/2011) |
SOUTH CAROLINA DEPARTMENT OF HEALTH AND ENVIRONMENTAL CONTROL |