
LICENSEE can be filled in online with ease. Simply open FormsPal PDF editing tool to finish the job without delay. In order to make our editor better and more convenient to utilize, we continuously come up with new features, considering suggestions from our users. With some easy steps, you'll be able to begin your PDF editing:
Step 1: Simply hit the "Get Form Button" at the top of this page to get into our form editing tool. There you'll find all that is necessary to fill out your document.
Step 2: With our handy PDF file editor, you could do more than just fill out blank form fields. Express yourself and make your docs look great with customized text added in, or optimize the file's original content to excellence - all comes along with an ability to insert your personal images and sign the document off.
This form will require specific data to be filled in, thus be certain to take your time to fill in exactly what is asked:
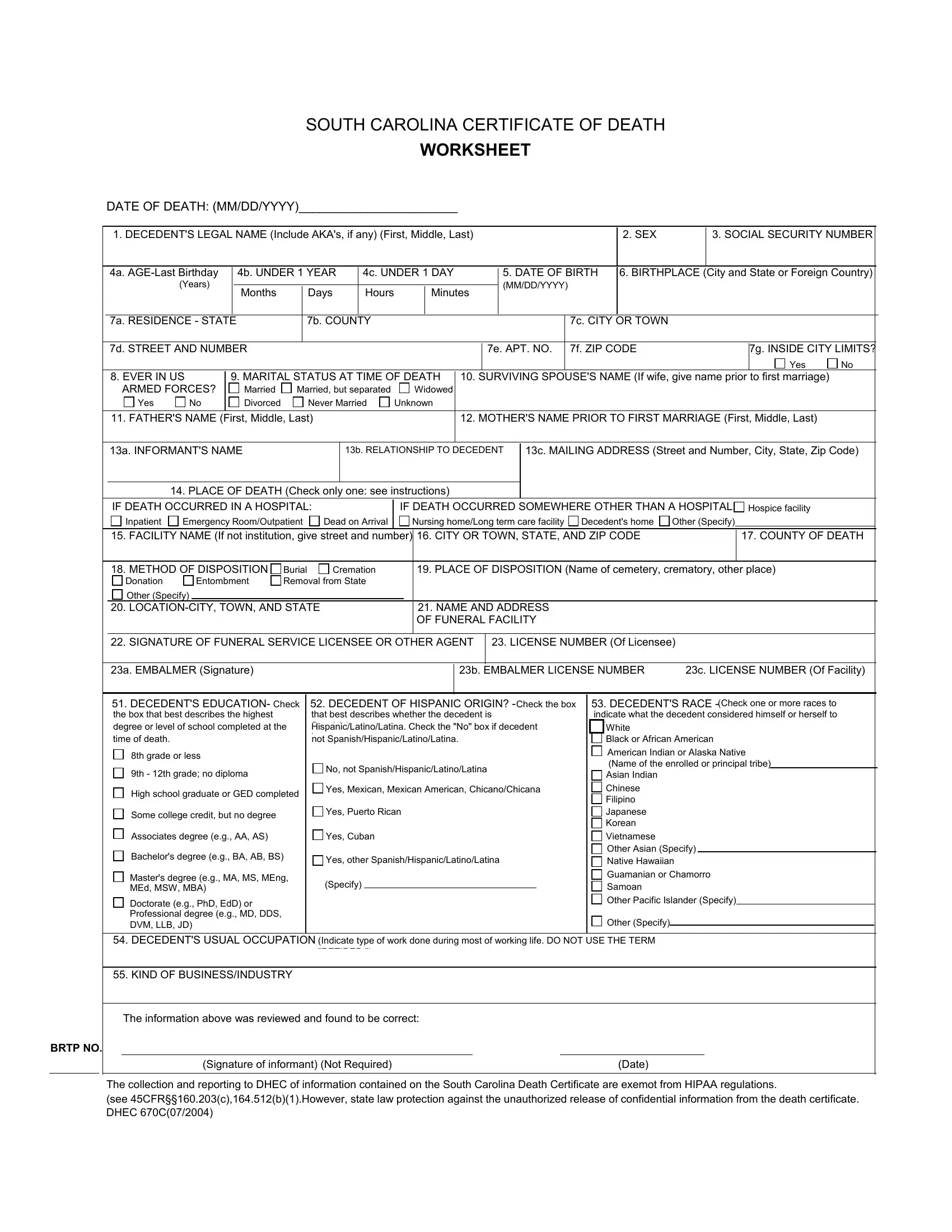
1. While submitting the LICENSEE, make certain to include all necessary blank fields within the associated section. It will help facilitate the process, allowing for your information to be processed without delay and properly.
2. When the last array of fields is done, you'll want to add the necessary details in DECEDENTS EDUCATION the box that, Check, th grade or less, th th grade no diploma, DECEDENT OF HISPANIC ORIGIN that, i h, Check the box, No not SpanishHispanicLatinoLatina, Check one or more races to, Black or African American, American Indian or Alaska Native, High school graduate or GED, Yes Mexican Mexican American, Some college credit but no degree, and Yes Puerto Rican so that you can move on further.
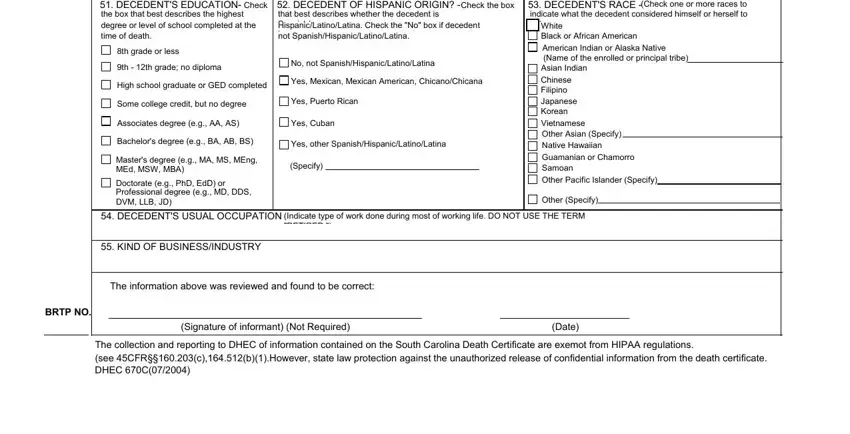
People who use this form frequently get some points wrong when filling out th th grade no diploma in this area. Make sure you re-examine everything you type in here.
Step 3: Look through the details you have typed into the blanks and click the "Done" button. Sign up with FormsPal today and immediately access LICENSEE, ready for downloading. All adjustments you make are saved , which enables you to change the form at a later time if required. FormsPal is invested in the confidentiality of our users; we make certain that all personal data put into our tool remains protected.