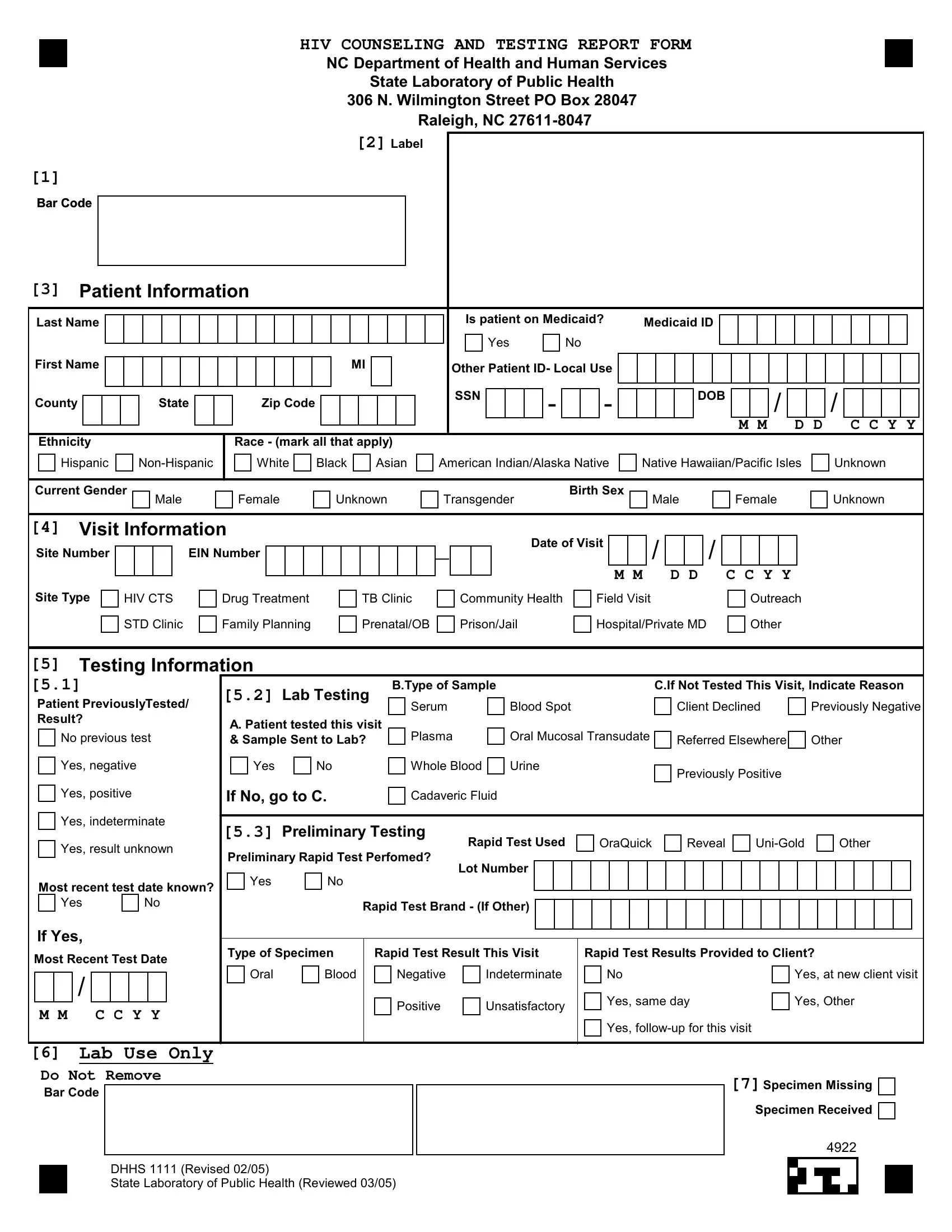
The DHHS 1111 form, integral to the North Carolina Department of Health and Human Services and the State Laboratory of Public Health's efforts to track and manage HIV testing and counseling, embodies a comprehensive tool for gathering critical patient and test information. This form captures a broad spectrum of data starting from basic patient demographics, including name, ethnicity, race, and Medicaid status, to more detailed visit and testing information such as the type and site of visit, reasons for not testing if applicable, and details about any preliminary testing conducted. It also delves into the specifics of lab testing, asking whether the patient was tested during the visit, the type of specimen collected if tested, and the results of any rapid tests conducted. The form is meticulously designed to ensure that patients receive appropriate pre-test counseling, with sections dedicated to capturing whether counseling was provided and if informed consent for testing was obtained. Additionally, it touches on sensitive areas such as pregnancy status in female patients and risk behaviors that might influence an individual's HIV risk profile. By requiring detailed documentation on whether a patient has been previously tested for HIV and the results of those tests, the form plays a crucial role in preventing duplicate testing while ensuring continuity of care. This structured document not only facilitates a systematic approach to HIV counseling and testing but also aids in the collection of vital statistics to monitor and address the HIV/AIDS epidemic in North Carolina.
| Question | Answer |
|---|---|
| Form Name | Form Dhhs 1111 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | HIV_NC_CTR_form state farm consent to rate form |
HIV COUNSELING AND TESTING REPORT FORM
NC Department of Health and Human Services
State Laboratory of Public Health
306 N. Wilmington Street PO Box 28047
Raleigh, NC
[2] Label
[1]
Bar Code
[3]Patient Information
Last Name
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MI |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
County |
|
|
|
|
|
State |
|
|
|
|
|
|
Zip Code |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Ethnicity |
|
|
|
|
|
|
|
|
|
|
Race - (mark all that apply) |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
Hispanic |
|
|
|
|
White |
Black |
|
|
Asian |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Is patient on Medicaid? |
|
Medicaid ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
Other Patient ID- Local Use |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
SSN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
- |
|
|
- |
|
|
|
|
DOB |
|
|
|
|
/ |
|
|
|
|
/ |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M M |
|
|
|
D D |
|
|
|
C C Y Y |
|
||||||||||
American Indian/Alaska Native |
|
Native Hawaiian/Pacific Isles |
|
Unknown |
|
||||||||||||||||||||||||||||||||
Current Gender |
|
|
|
Birth Sex |
|
|
Male |
Female |
Unknown |
Transgender |
Male |
Female |
Unknown |
[4] Visit Information |
|
|
|
|
|
|
|
|
|
|
|
|
Date of Visit |
|
|
/ |
|
|
/ |
|
|
|
|
||||
Site Number |
|
|
|
EIN Number |
|
|
|
|
|
|
|
|
|
__ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M M |
|
D D |
|
C C Y Y |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Site Type
HIV CTS STD Clinic
Drug Treatment Family Planning
TB Clinic Prenatal/OB
Community Health Prison/Jail
Field Visit Hospital/Private MD
Outreach Other
[5]Testing Information
[5.1]
Patient PreviouslyTested/ Result?
No previous test
Yes, negative
Yes, positive
Yes, indeterminate
[5.2] Lab Testing
A. Patient tested this visit & Sample Sent to Lab?
Yes |
No |
If No, go to C.
B.Type of Sample |
|
C.If Not Tested This Visit, Indicate Reason |
|
Serum |
Blood Spot |
Client Declined |
Previously Negative |
Plasma |
Oral Mucosal Transudate |
Referred Elsewhere |
Other |
|
|
||
Whole Blood |
Urine |
Previously Positive |
|
|
|
|
|
Cadaveric Fluid |
|
|
|
Yes, result unknown
Most recent test date known?
Yes |
No |
If Yes,
Most Recent Test Date
/
M M C C Y Y
[5.3] Preliminary Testing |
Rapid Test Used |
|
|
OraQuick |
|
Reveal |
|
Other |
|||||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||||
Preliminary Rapid Test Perfomed? |
Lot Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Rapid Test Brand - (If Other) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Specimen |
Rapid Test Result This Visit |
|
Rapid Test Results Provided to Client? |
|
|
|
|
|
|
||||||||||||||||||
Oral |
Blood |
Negative |
Indeterminate |
|
|
No |
|
|
|
|
|
|
|
Yes, at new client visit |
|||||||||||||
|
|
Positive |
Unsatisfactory |
|
|
Yes, same day |
|
|
Yes, Other |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
Yes, |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
[6]Lab Use Only
Do Not Remove
Bar Code
DHHS 1111 (Revised 02/05)
State Laboratory of Public Health (Reviewed 03/05)
[7]Specimen Missing
Specimen Received
4922
HIV COUNSELING AND TESTING REPORT FORM
NC Department of Health and Human Services
State Laboratory of Public Health
306 N. Wilmington Street PO Box 28047
Raleigh, NC
Bar Code
[8]
Pretest Counselor
Client Counseled
Yes |
No |
STARHS Consent
Yes |
No |
If Female, Is Patient Pregnant?
Yes |
No |
Unknown |
If Pregnant, In Prenatal Care
Yes |
Refused to Answer |
No |
Not Asked |
Outreach Venue?
Yes |
No |
Reason for the Visit - (mark all that apply)
Symptomatic for HIV/AIDS |
|
TB Related |
Risk Behaviors within the last 12 months - (mark all that apply)
Sex with man |
Child of HIV infected woman |
Client Referral |
|
Court Ordered |
Provider Referral |
|
Immigrant/Travel Req |
|
||
STD Related |
|
Occupational Exposure |
|
||
Drug Trmt Related |
|
Retest |
|
||
Family PL Related |
|
Requesting HIV Test |
|
||
PreNatal/OB Related |
|
Other |
|
Sex with woman
Injection Drug Use
Sex with HIV+ person
Sex with IDU
Sex with MSM
Sex in exchange for drugs/money Current STD diagnosis
Sex while using
Sex with other HIV/Aids Risk
Hemophilia/Blood Recipient
Health Care Exposure
Victim of Sexual Assault
No acknowledged Risk Other Risk
Primary Language
English
Local Use Field 1
Spanish
[9]Additional Demographic Information
Other Primary Language
Other
[10]Local Use Data Fields
Local Use Field 2 |
|
Local Use Field 3 |
|
Local Use Field 4 |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4922 |