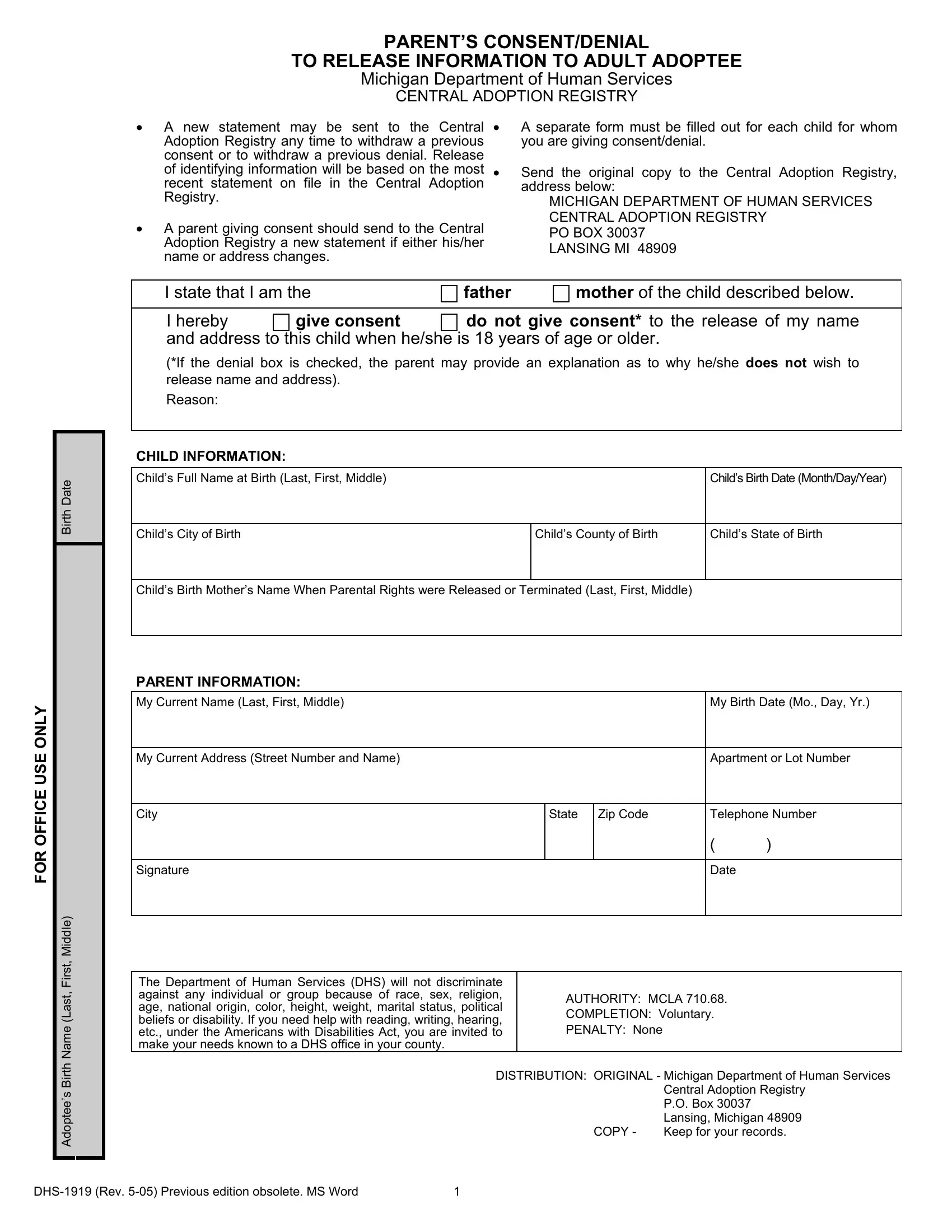
When it comes to the delicate intersection of adoption records and personal privacy, the Michigan Department of Human Services (DHS) has instituted a comprehensive process through its Central Adoption Registry, enabling parents to manage the disclosure of their identifying information to their adult adoptee children. This crucial procedure is encapsulated in the DHS form, specifically designed to either consent to or deny the release of a parent's name and address to their child once they reach 18 years of age. Parents hold the prerogative to update or withdraw their consent or denial at any point, a testament to the dynamic nature of familial relationships and personal circumstances. The necessity to submit a separate form for each child underscores the personalized approach taken by the Central Adoption Registry towards each adoption case. Detailed within the form are sections for the adoptee's birth information, including name, date, and place of birth, as well as comprehensive parent information. The form meticulously outlines the submission process, emphasizing the importance of keeping an updated record to facilitate or restrict future contact. This effort by the DHS to balance the rights and privacy concerns of both parents and adoptees illustrates a nuanced approach to a complex matter, ensuring that the process is both respectful and adaptable to the evolving needs of families.
| Question | Answer |
|---|---|
| Form Name | Form Dhs 1919 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | FIA1919_10574_7 form dhs 1919 |
PARENT’S CONSENT/DENIAL
TO RELEASE INFORMATION TO ADULT ADOPTEE
Michigan Department of Human Services
CENTRAL ADOPTION REGISTRY
•A new statement may be sent to the Central Adoption Registry any time to withdraw a previous consent or to withdraw a previous denial. Release of identifying information will be based on the most recent statement on file in the Central Adoption Registry.
•A parent giving consent should send to the Central Adoption Registry a new statement if either his/her name or address changes.
•A separate form must be filled out for each child for whom you are giving consent/denial.
•Send the original copy to the Central Adoption Registry, address below:
MICHIGAN DEPARTMENT OF HUMAN SERVICES CENTRAL ADOPTION REGISTRY
PO BOX 30037 LANSING MI 48909
FOR OFFICE USE ONLY
Birth Date |
Adoptee’s Birth Name (Last, First, Middle)
I state that I am the |
father |
|
mother of the child described below. |
||||||
|
|
|
|
|
|
|
|
||
I hereby |
give consent |
do not give consent* to the release of my name |
|||||||
and address to this child when he/she is 18 years of age or older. |
|
|
|
||||||
(*If the denial box is checked, the parent may provide an explanation as to why he/she does not wish to |
|||||||||
release name and address). |
|
|
|
|
|
|
|
|
|
Reason: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHILD INFORMATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Child’s Full Name at Birth (Last, First, Middle) |
|
|
|
|
|
|
Child’s Birth Date (Month/Day/Year) |
||
|
|
|
|
|
|
|
|
|
|
Child’s City of Birth |
|
|
|
Child’s County of Birth |
|
Child’s State of Birth |
|||
|
|
|
|
|
|
|
|||
Child’s Birth Mother’s Name When Parental Rights were Released or Terminated (Last, First, Middle) |
|
||||||||
|
|
|
|
|
|
|
|
|
|
PARENT INFORMATION: |
|
|
|
|
|
|
|
|
|
My Current Name (Last, First, Middle) |
|
|
|
|
|
|
My Birth Date (Mo., Day, Yr.) |
||
|
|
|
|
|
|
|
|
||
My Current Address (Street Number and Name) |
|
|
|
|
|
|
Apartment or Lot Number |
||
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
State |
Zip Code |
|
Telephone Number |
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
Signature |
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
The Department of Human Services (DHS) will not discriminate |
|
|
|
|
|
|
|
||
against any individual or |
group because of race, sex, |
religion, |
|
|
AUTHORITY: MCLA 710.68. |
|
|||
age, national origin, color, height, weight, marital status, political |
|
|
|
||||||
|
|
COMPLETION: Voluntary. |
|
||||||
beliefs or disability. If you need help with reading, writing, hearing, |
|
|
|
||||||
|
|
PENALTY: None |
|
|
|
||||
etc., under the Americans with Disabilities Act, you are invited to |
|
|
|
|
|
||||
make your needs known to a DHS office in your county. |
|
|
|
|
|
|
|
|
|
|
|
DISTRIBUTION: ORIGINAL - Michigan Department of Human Services |
|||||||
|
|
|
|
|
|
|
Central Adoption Registry |
||
|
|
|
|
|
|
|
P.O. Box 30037 |
|
|
|
|
|
|
|
|
|
Lansing, Michigan 48909 |
||
|
|
|
|
|
|
COPY - |
Keep for your records. |
||
1 |