DL-15 (10-18)
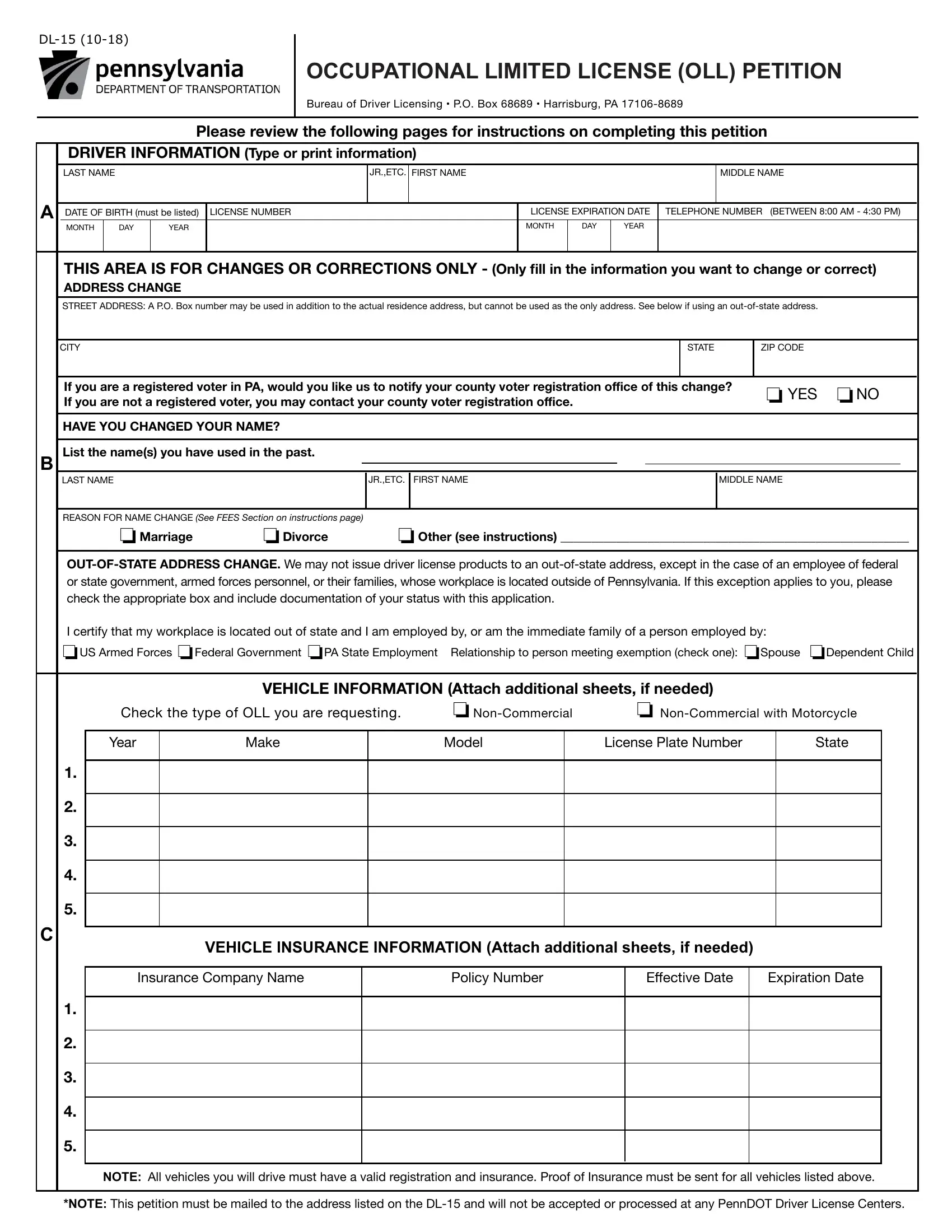
OCCUPATIONAL LIMITED LICENSE (OLL) PETITION
Bureau of Driver Licensing • P.O. Box 68689 • Harrisburg, PA 17106-8689
Please review the following pages for instructions on completing this petition
DRIVER INFORMATION (Type or print information)
|
|
LAST NAME |
|
|
|
JR.,ETC. |
FIRST NAME |
|
|
|
|
|
|
MIDDLE NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A DATE OF BIRTH (must be listed) |
LICENSE NUMBER |
|
|
LICENSE EXPIRATION DATE |
TELEPHONE NUMBER (BETWEEN 8:00 AM - 4:30 PM) |
|
|
|
MONTH |
DAY |
YEAR |
|
|
|
|
MONTH |
|
DAY |
|
YEAR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
THIS AREA IS FOR CHANGES OR CORRECTIONS ONLY - (Only ill in the information you want to change or correct) |
|
|
|
ADDRESS CHANGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS: A P.O. Box number may be used in addition to the actual residence address, but cannot be used as the only address. See below if using an out-of-state address. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If you are a registered voter in PA, would you like us to notify your county voter registration oice of this |
change? |
❏ YES |
❏NO |
|
|
|
If you are not a registered voter, you may contact your county voter registration oice. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HAVE YOU CHANGED YOUR NAME? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B List the name(s) you have used in the past. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
|
|
JR.,ETC. |
FIRST NAME |
|
|
|
|
|
|
MIDDLE NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REASON FOR NAME CHANGE (See FEES Section on instructions page) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏Marriage |
❏Divorce |
❏ Other (see instructions) ________________________________________________________ |
|
OUT-OF-STATE ADDRESS CHANGE. We may not issue driver license products to an out-of-state address, except in the case of an employee of federal or state government, armed forces personnel, or their families, whose workplace is located outside of Pennsylvania. If this exception applies to you, please check the appropriate box and include documentation of your status with this application.
I certify that my workplace is located out of state and I am employed by, or am the immediate family of a person employed by:
❏US Armed Forces ❏Federal Government ❏PA State Employment Relationship to person meeting exemption (check one): ❏Spouse ❏Dependent Child
VEHICLE INFORMATION (Attach additional sheets, if needed)
Check the type of OLL you are requesting. |
❏ Non-Commercial |
❏ Non-Commercial with Motorcycle |
|
|
|
|
|
Year |
Make |
Model |
License Plate Number |
State |
1.
2.
3.
4.
5.
C
VEHICLE INSURANCE INFORMATION (Attach additional sheets, if needed)
Insurance Company Name |
Policy Number |
Efective Date |
Expiration Date |
1.
2.
3.
4.
5.
NOTE: All vehicles you will drive must have a valid registration and insurance. Proof of Insurance must be sent for all vehicles listed above.
*NOTE: This petition must be mailed to the address listed on the DL-15 and will not be accepted or processed at any PennDOT Driver License Centers.
DL-15 (10-18)
|
|
EMPLOYER INFORMATION (W1) |
SCHOOL INFORMATION (S1) |
MEDICAL TREATMENT INFORMATION (T) |
|
|
|
|
|
|
|
|
(Attach additional sheets if you have more than one job.) |
School Name _______________________________ |
|
|
|
Company Name ___________________________ |
Provider Name ____________________________ |
|
Address ___________________________________ |
Address ____________________________________ |
Address ___________________________________ |
|
City _______________________________________ |
City ________________________________________ |
City _______________________________________ |
|
State_________________ Zip _________________ |
State _____________________ Zip ______________ |
State _____________________ Zip _____________ |
|
Telephone Number of your immediate Supervisor: |
Dean's Name ________________________________ |
Contact Name_______________________________ |
|
_________________________________ |
Telephone Number of your Dean: |
Telephone Number: |
|
Self Employed: ❒ Yes ❒ No |
|
____________________________________ |
______________________________________ |
|
|
(Submit proof of self-employment with OLL |
|
|
|
|
|
|
Petition by sending a copy of your 1099 form) |
|
|
|
|
|
|
|
|
|
|
|
|
EXPLANATION |
|
|
|
|
Explain your need for an OLL in detail, including why an OLL is essential to your occupation, work, trade, |
|
|
treatment, or study. Be sure to outline the hours and days of the week you need to drive. Attach additional |
D |
|
sheets of paper if needed. *Note: This petition must be mailed to the address listed on the DL-15 and will not be |
|
|
accepted or processed at any PennDOT Driver License Centers. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The driver shall only operate a designated vehicle as deined in 75 Pa.C.S. § 1553(f)
ACKNOWLEDGMENT
❏For Veterans wishing to add the Veterans Designation to their Driver’s License or ID Card: I certify under penalty of law that I am a qualiied applicant and hereby request it be added to my product. I understand that misrepresentation will result in the cancellation of my driver’s license.
I acknowledge that receiving a Pennsylvania Permit, License or ID card will cancel or invalidate any Permit, License or ID card from another state. I certify under penalty of law that all information given on this Petition is true and correct. I understand that the $68.00 Petition fee is non-refundable. I conirm that I have received notice of the provisions of Section 3709 of the Vehicle Code.
❏I used a Messenger Service to assist me in completing this form. I authorize the Department to give this Messenger
EService my driving record information.
❏I wish to contribute $1.00 to the Organ Donation Awareness Trust Fund (See instructions)
❏I wish to contribute $3.00 to the Veterans’ Trust Fund (VTF) (See instructions)
SIGNX
HERE
APPLICANT'S SIGNATURE IN INK |
DATE |
WARNING: Misstatement of fact is a misdemeanor of the third degree punishable by a ine of up to $2,500 and/or imprisonment up to one year (18 Pa C.S., Section 4904[b]).
|
|
CHECKLIST |
SEND BY CERTIFIED MAIL TO: |
|
Did you remember to include the following fees on your check or money order? |
|
|
1. |
❏ Proof of Insurance for all vehicles listed in the Petition. (Required) |
PA Department of Transportation |
|
2. |
❏ Renewal Fee and DL-143 Application (contact Department for fees if your license |
Bureau of Driver Licensing |
|
|
is expired or will expire during your term of suspension) (Required) |
|
|
OLL/PL Unit |
|
3. |
❏ Restoration Fee (Required) For amount, call 717-412-5300 (amount is in |
|
|
restoration letter.) |
P.O. Box 68689 |
|
4. |
❏ $68.00 OLL Petition Fee (non-refundable) (Required) |
|
Harrisburg, PA 17106-8689 |
|
5. |
❏ $3.00 contribution to the Veterans’ Trust Fund (Optional) |
|
|
|
6. |
❏ $1.00 contribution to the Organ Donation Awareness Trust Fund (Optional) |
(THIS FORM MUST BE MAILED TO THE |
|
ADDRESS ABOVE, PLEASE DO NOT |
|
7. |
❏ $ ___________________________ TOTAL AMOUNT DUE WITH PETITION |
|
BRING TO DRIVER LICENSE CENTER) |
|
|
|
|
DL-15 (10-18)
OCCUPATIONAL LIMITED LICENSE INSTRUCTIONS AND PETITION
What is an Occupational Limited License?
An Occupational Limited License (OLL) is a driver’s license issued to a driver whose Pennsylvania driving privilege has been, or will be, suspended. An OLL authorizes driving a designated motor vehicle, under certain conditions, when it is necessary for the driver’s occupation, work, trade, medical treatment or study. Based on your driving record and violations, the PA Department of Transportation will evaluate whether or not you are eligible for an OLL based on section 1553 of the Pennsylvania Vehicle Code which can be found at http://www.legis.state.pa.us/cfdocs/legis/LI/consCheck.cfm?txtType =HTM&ttl=75&div=0&chpt=15.
To assist potential applicants an Occupational Limited License Fact Sheet can be used and you may obtain a copy from our website (http://www.dot.state. pa.us/Public/DVSPubsForms/BDL/BDL%20Fact%20Sheets/fs-oll.pdf). Certain violations and offenses make you ineligible for an OLL that are outlined on the OLL Fact Sheet. Once you decide to apply you must do so by completing the attached Occupational Limited License Petition (form DL-15).
To have continuous driving privileges, you must send your completed OLL Petition, check or money order, and Proof of Insurance(s) by certiied mail to the PA Department of Transportation at least 20 days before your suspension begins. Within 20 days of receiving your Petition, the Department will inform
you in writing whether or not you qualify for an OLL. This correspondence may take an additional 7 days to arrive through the mail to you. Your current license must be surrendered to the Department during this time. Petitions must be sent by certiied mail.
If your Petition is received and approved less than 15 days but the OLL has not been issued before your suspension begins, the Department will delay the
start of your suspension for up to 15 days. You will be issued an interim (temporary) license that is valid until the new suspension start date. Your suspen- sion will begin upon the new effective date. You need to send your current driver’s license, by certiied mail, to the address shown on the bottom of the
Petition.
If you are already under suspension and do not have a valid license, complete and send the attached Petition with a check or money order made payable to PA Department of Transportation, and Proof of Insurance(s) by certiied mail to the address shown at the bottom of the Petition. Within 20 days of
receiving your Petition, the Department will inform you in writing whether or not you are eligible for an OLL. This correspondence may take an additional 7 days to arrive through the mail to you.
INSTRUCTIONS FOR COMPLETING THE PETITION
Carefully read and follow the instructions below for completing the attached OLL Petition. The Petition must be complete and accurate for your request to be considered. Attach additional sheets of paper if needed.
1.SECTION A - Fill in all blocks. If you do not know your license number or expiration date, please leave those blocks blank.
Provide a daytime telephone number (between 8:00 a.m. and 4:30 p.m. Monday through Friday) where the Department can reach you, if necessary, to get additional information to process your Petition.
2.SECTION B - Name Change - If you desire to use your birth name, you must present a copy of your state issued birth certiicate with a raised seal. If your name was changed by permission of court, you must present a Certiied Copy of the Court Order. If you desire to use your spouse’s surname, you must present your marriage certiicate. If you desire to use another name, you must present your Social Security Card, together with two other sources issued in the desired name such as Tax Records, Selective Service Card, Voter Registration Card, Passport, any form of Photo I.D. issued by a governmental agency, or state issued Birth Certiicate. All additional documents for this section must be notarized copies.
To report errors on your driver’s license relating to name, date of birth or social security number, please contact PennDOT’s Customer Care Center at 717-412-5300.
If you are required to present supporting documentation to correct your record, all documents must be originals and presented in person at a PennDOT Driver License Center.
•For NAME corrections, you must present your state issued birth certiicate with a raised seal, a Certiied Copy of the Court Order or your marriage certiicate.
•For DATE OF BIRTH corrections, you must present state issued birth certiicate with raised seal.
•For SOCIAL SECURITY NUMBER corrections, you must present your Social Security Card.
*Note: All name changes must be made in person at a Driver License Center. All documents must be original.
3.SECTION C - Check only one box to indicate the type of Occupational Limited License you are applying for. Commercial drivers cannot get an OLL to drive a commercial vehicle. A commercial driver could be eligible for an OLL to drive a non-commercial vehicle to and from work or during work. A school bus cannot be driven by someone with an OLL. List all vehicles (including rental vehicles) that you will drive between your home and work, school, or treatment facility and during work or school. For each vehicle that you list, give the year/ make/model of the vehicle, the license plate number and state, the vehicle insurance company name, policy number, and the policy’s efective and expiration dates. You must also send a copy (not the original) of one of the following documents, for each vehicle listed, as proof of inancial responsibility/insurance along with the Petition:
(1)A inancial responsibility/insurance identiication card
(2)A copy of the declaration page from the insurance policy
(3)A copy of an application for insurance to the Pennsylvania Automobile Insurance Plan signed by a licensed insurance agent or broker
(4)A certiicate of self-insurance issued by the Pennsylvania Department of Transportation
(5)A valid binder of insurance issued by an insurance agent or company licensed to sell motor vehicle liability insurance in Pennsylvania if you drive more than one company-owned vehicle, you only need to send one copy of the company’s inancial responsibility/insurance identiication card.
4.SECTION D - Provide the requested information for your employer, school, or treatment center, or any combination depending on where you need to drive. If you have more than one job, or attend more than one school, attach a piece of paper that lists the same information asked in this section for each additional job or school.
5.SECTION E - Read this section before signing. Once you have read and understand the information, sign your name in ink on the line provided. Your Petition will be rejected if it does not include your signature. If you used a Messenger Service, such as an automobile club or notary public, to help you complete the Petition, place a check in the box provided.
Veterans Designation: You have the opportunity to add the veterans designation to your driver’s license, which clearly indicates you are a veteran of the United States Armed Forces. To qualify, you must have served in the United States Armed Forces, including a reserve component or the National Guard, and have been discharged or released from such service under conditions other than dishonorable. If you are requesting to add the veterans designation to your license, make sure you check the box at the top in Section F.
Veterans’ Trust Fund (VTF): You have the opportunity to make a tax deductible contribution to the VTF. Your contribution will help support programs and projects for Pennsylvania veterans and their families. Since this additional $3.00 is not part of the fee, please add the donated amount to your payment. Also, please check the proper block on the form to ensure your contribution is handled properly.
Organ Donation Awareness Trust Fund (ODTF): You have the opportunity to contribute $1.00 to the Fund. The additional $1.00 contribution must be added to your payment. You must also check the block provided to ensure proper handling of your contribution. The ODTF provides for the development and implementation of donor awareness programs and funds shall be appropriated subject to the approval of the Governor.
6.Once you have completed the petition, to calculate the fee payable to PennDOT, by reviewing the checklist at the bottom of the DL-15 form. You will need to pay the $68 non-refundable application fee, a restoration fee, and, if your current license expires during the term of your suspension, the license renewal fee. To determine the restoration fee you owe, you will need to call 717-412-5300 and ask for the fee amount from your restoration letter. The license renewal fee will vary depending on the type of license you hold. If you hold a Class C non-commercial license, the renewal fee is $30.50. Please note, to qualify for an Occupational Limited License, you must have paid all ines and court costs to the judicial system. These payments should not be sent to PennDOT. Once you have reviewed the check list and calculated what you owe to PennDOT, send a check or money order in that exact amount made payable to the PA Department of Transportation along with the DL-15 petition form and proof of insurance by certiied mail to the PA Department of Transportation, Bureau of Driver Licensing, OLL/PL Unit, P.O. Box 68689, Harrisburg, PA 17106-8689.
7.Complete the Limited License Aidavit (DL-15A) forms. You are required by law to complete a Limited License Aidavit and carry it with your Photo Limited License at all times. An Aidavit Form is attached to this petition. You may start the process of completing it while awaiting to receive your limited license camera card.
For Sections C, D, and/or E indicate each destination, time of day, and the days of the week that the schedule applies. Examples have been given for you to follow. If needed, attach additional sheets of paper explaining your driving schedule. If you do not have a routine driving schedule due to your job duties (such as self-employed, salespersons, delivery or truck drivers), include an explanation of the territory, or area, that you drive from and to along with your detailed explanation for an OLL. Be as speciic as possible. You must list days and hours you work.
If you have any questions, please write to the PA Department of Transportation and send to: PA Department of Transportation, Bureau of Driver Licensing, OLL/PL Unit .O. Box 68689, Harrisburg, PA 17106-8689. In order to provide an immediate response, please include your daytime telephone number.
PROVISIONS OF SECTION 3709 OF THE VEHICLE CODE
Section 3709 provides for a ine of up to $300 for dropping, throwing or depositing, upon any highway, or upon any other public or private property without the consent of the owner thereof or into or on the waters of this Commonwealth, from a vehicle, any waste paper, sweepings, ashes, household waste, glass, metal, refuse or rubbish or any dangerous or detrimental substance, or permitting any of the preceding without immediately removing such items or causing their removal.
For any violation of Section 3709, I may be subject to a ine of up to $300 upon conviction, including any violation resulting from the conduct of any other persons present within any vehicle of which I am the driver.
DL-15A (12-15)
LIMITED LICENSE AFFIDAVIT
FOR LAW ENFORCEMENT OFFICIALS: This Aidavit allows this person to drive the vehicle(s) listed during the stated times for work, school, or medical treatment. in conjunction with an Occupational Limited License and under section 1553 of the PA Vehicle Code.
CARRY THIS AFFIDAVIT WITH YOUR LIMITED LICENSE AT ALL TIMES.
|
DRIVER INFORMATION (Type or print information) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
|
|
|
|
JR.,ETC. |
FIRST NAME |
|
|
MIDDLE NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
DATE OF BIRTH (must be listed) |
|
LICENSE NUMBER |
|
|
|
|
|
|
|
|
|
LICENSE EXPIRATION DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
DAY |
YEAR |
|
|
|
|
|
|
|
|
|
|
MONTH |
|
|
DAY |
|
YEAR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CURRENT STREET ADDRESS A Post Oice Box number may be used in addition to the actual residence |
CITY |
|
|
|
|
|
STATE |
ZIP CODE |
|
address, but cannot be used as the only address. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year |
|
|
Make |
|
|
|
Model |
|
License Plate Number |
|
|
State |
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE INSURANCE INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance Company Name |
|
|
|
Policy Number |
|
Efective Date |
|
Expiration Date |
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVING SCHEDULE INSTRUCTIONS
List your daily driving schedule. If you have a routine driving schedule, complete the chart(s) using the Destination Codes listed to the left of the chart. If you do not have a routine driving schedule due to your job duties (such as salespersons, delivery and truck drivers), explain the territory or area you drive, along with the days and hours you work. For both routine and non-routine schedules, include a detailed explanation of your need for an OLL on the lines marked Detailed Explanation.
WORK DRIVING SCHEDULE
EMPLOYER INFORMATION (W1)
(Complete additional aidavits if you have more than one job.)
Company Name ______________________________
Address _____________________________________
City _________________________________________
State ________________ Zip ___________________
Supervisor's Name_____________________________
EXAMPLE
Destination Codes
W1 = Primary Job
W2 = Second Job
W3 = Third Job
H = Home
Detailed Explanation
Leave |
Time |
AM PM |
|
|
|
|
H |
7:30 |
4 |
|
W1 |
5:00 |
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Arrive |
Time |
AM PM |
|
|
|
|
W1 |
8:00 |
4 |
|
H |
5:30 |
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mo Tu We Th Fr Sa Su
4 4 4 4
4 4 4 4
Telephone Number of your immediate Supervisor:
_______________________________________
Self Employed: ❒ Yes ❒ No
EMPLOYER ACKNOWLEDGMENT
I certify under penalty of law that all information given on this Afidavit is true and correct.
|
|
|
Employer Signature in ink |
|
Date |
|
WARNING: Misstatement of fact is a misdemeanor of the third degree punishable by a ine of up to $2,500 and/or imprisonment up to one year (18 Pa C.S., Section 4904[b]).