

Form Hca 15 can be filled in without any problem. Just make use of FormsPal PDF tool to complete the job promptly. To make our tool better and easier to use, we constantly develop new features, bearing in mind feedback coming from our users. To begin your journey, consider these easy steps:
Step 1: Click on the "Get Form" button above. It is going to open up our editor so that you could start filling out your form.
Step 2: Using our online PDF editor, you'll be able to do more than merely fill out blank fields. Try all of the features and make your docs seem professional with custom textual content added, or optimize the original content to perfection - all that comes along with the capability to incorporate just about any photos and sign it off.
With regards to the fields of this particular document, this is what you should do:
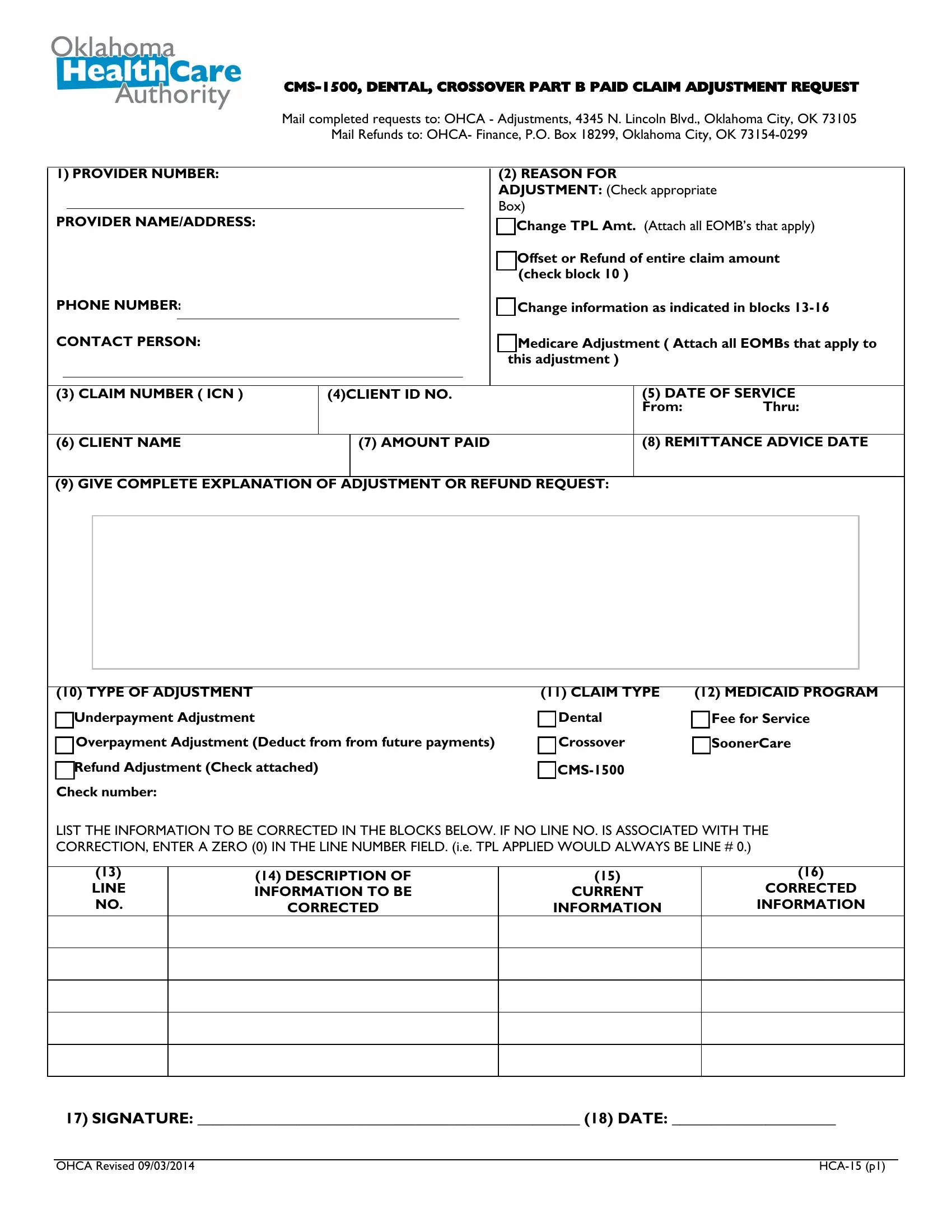
1. You will need to fill out the Form Hca 15 correctly, so be mindful while filling out the parts containing all these blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - TYPE OF ADJUSTMENT a Underpayment, CLAIM TYPE a Dental a Crossover, CMS, MEDICAID PROGRAM, Fee for Service SoonerCare, LIST THE INFORMATION TO BE, LINE NO, DESCRIPTION OF INFORMATION TO BE, CORRECTED, CURRENT, INFORMATION, CORRECTED INFORMATION, SIGNATURE DATE, OHCA Revised, and HCA p with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
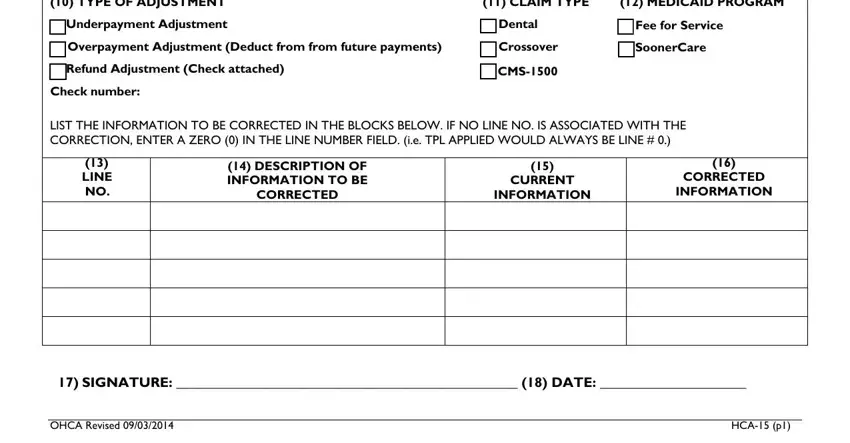
Be very attentive when filling out CMS and CLAIM TYPE a Dental a Crossover, because this is where a lot of people make mistakes.
Step 3: Once you have glanced through the details in the fields, click "Done" to complete your form. Sign up with us today and easily use Form Hca 15, available for download. Each and every modification made is handily kept , making it possible to change the pdf further if necessary. We do not share or sell any information that you type in whenever dealing with forms at our site.