
If you desire to fill out pa work license, you don't have to download any sort of programs - simply try our PDF editor. The editor is continually improved by us, receiving new awesome functions and turning out to be a lot more versatile. With just a few simple steps, you can start your PDF journey:
Step 1: Hit the "Get Form" button at the top of this page to get into our PDF tool.
Step 2: As soon as you start the tool, you will notice the document made ready to be filled in. Other than filling out various blank fields, you can also do many other actions with the file, particularly writing any words, changing the initial textual content, inserting graphics, affixing your signature to the PDF, and a lot more.
Be attentive while filling out this document. Make sure all mandatory blank fields are done properly.
1. Whenever filling in the pa work license, be certain to incorporate all necessary fields within the relevant section. It will help to hasten the work, which allows your information to be handled fast and properly.
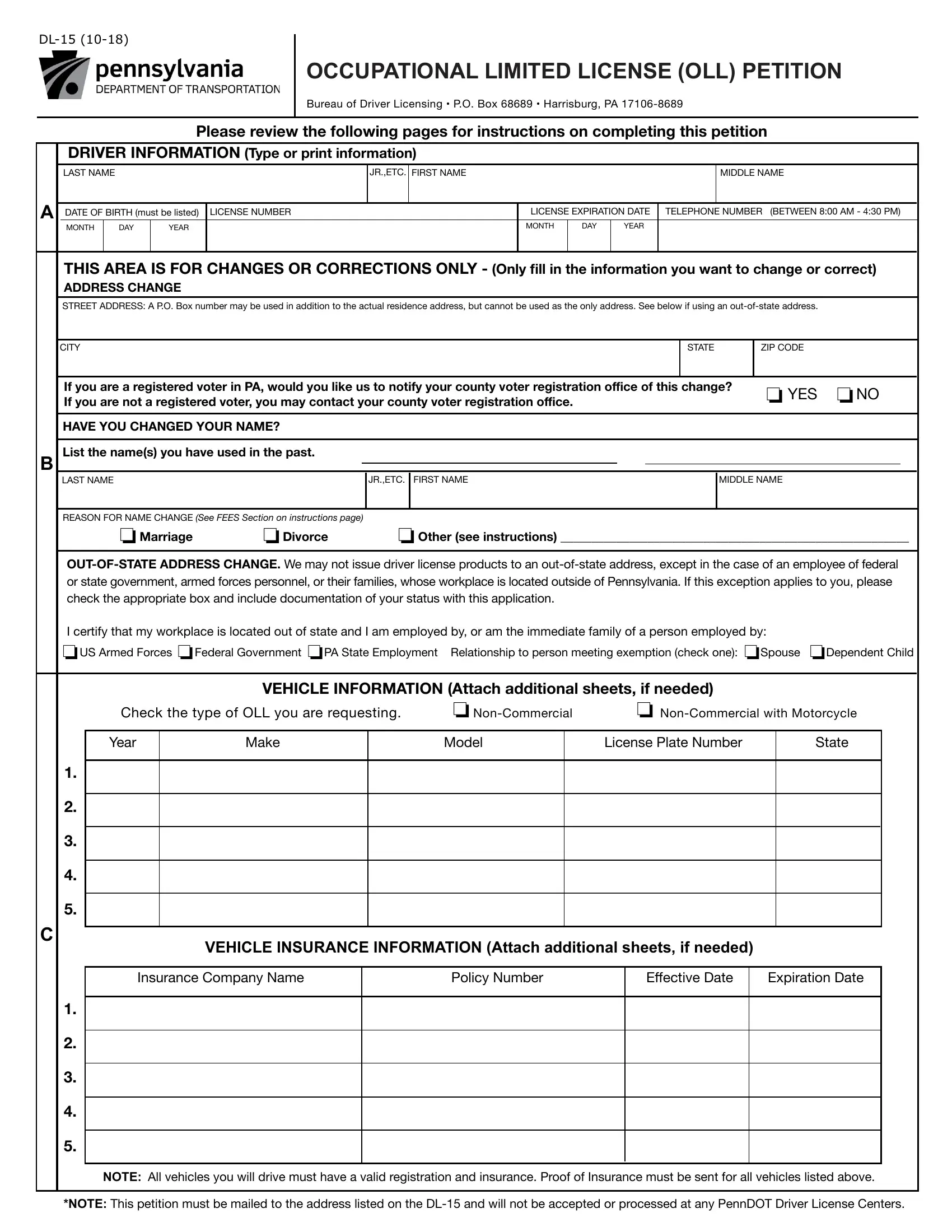
2. The next part would be to fill out all of the following blanks: VEHICLE INFORMATION Attach, Check the type of OLL you are, Model, Make, NonCommercial with Motorcycle, License Plate Number, VEHICLE INSURANCE INFORMATION, Insurance Company Name, Policy Number, Effective Date, and Expiration Date.
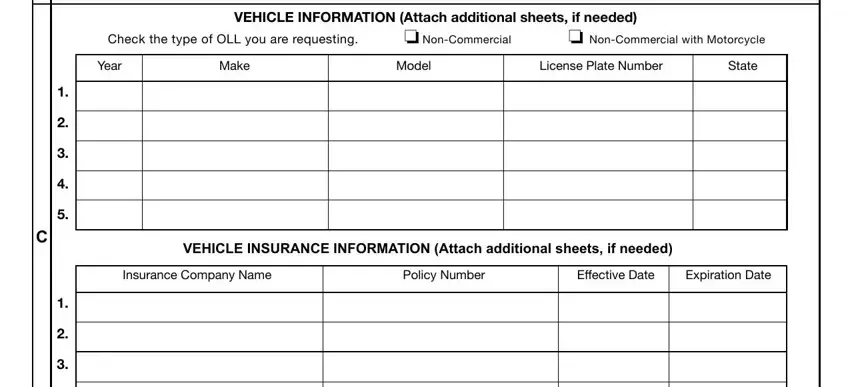
3. Your next stage is going to be simple - complete all the empty fields in NOTE All vehicles you will drive, and NOTE This petition must be mailed to conclude this process.

As to NOTE This petition must be mailed and NOTE This petition must be mailed, ensure you review things in this current part. Both these are thought to be the key fields in the file.
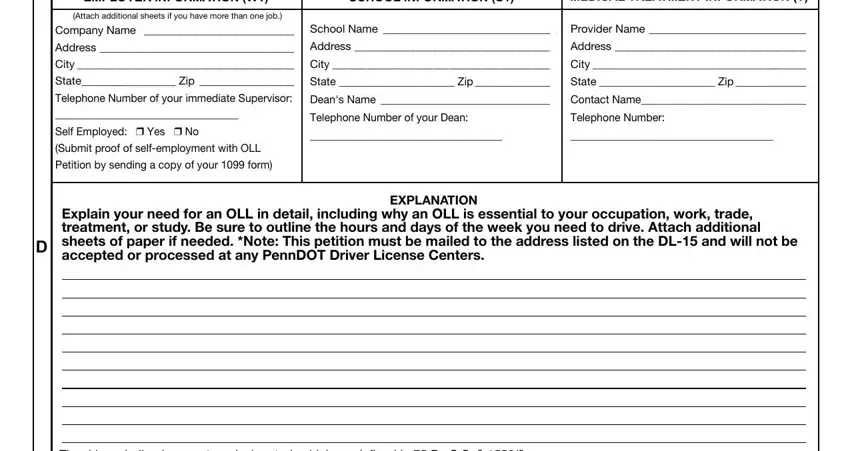
4. Now complete the next part! Here you will get these EMPLOYER INFORMATION W, SCHOOL INFORMATION S, MEDICAL TREATMENT INFORMATION T, Attach additional sheets if you, Company Name Address City State, School Name Address City State, Provider Name Address City, Explain your need for an OLL in, EXPLANATION, and The driver shall only operate a fields to do.
5. Since you approach the end of this file, you will find just a few more things to complete. In particular, The driver shall only operate a, ACKNOWLEDGMENT, For Veterans wishing to add the, I acknowledge that receiving a, I used a Messenger Service to, SIGN, HERE, WARNING Misstatement of fact is a, APPLICANTS SIGNATURE IN INK, DATE, CHECKLIST, SEND BY CERTIFIED MAIL TO, Did you remember to include the, is expired or will expire during, and PA Department of Transportation must be done.
Step 3: Immediately after going through your form fields you have filled in, press "Done" and you're all set! Sign up with us now and easily use pa work license, all set for downloading. All adjustments you make are preserved , allowing you to change the form at a later stage if necessary. We do not sell or share any information that you enter while working with forms at FormsPal.