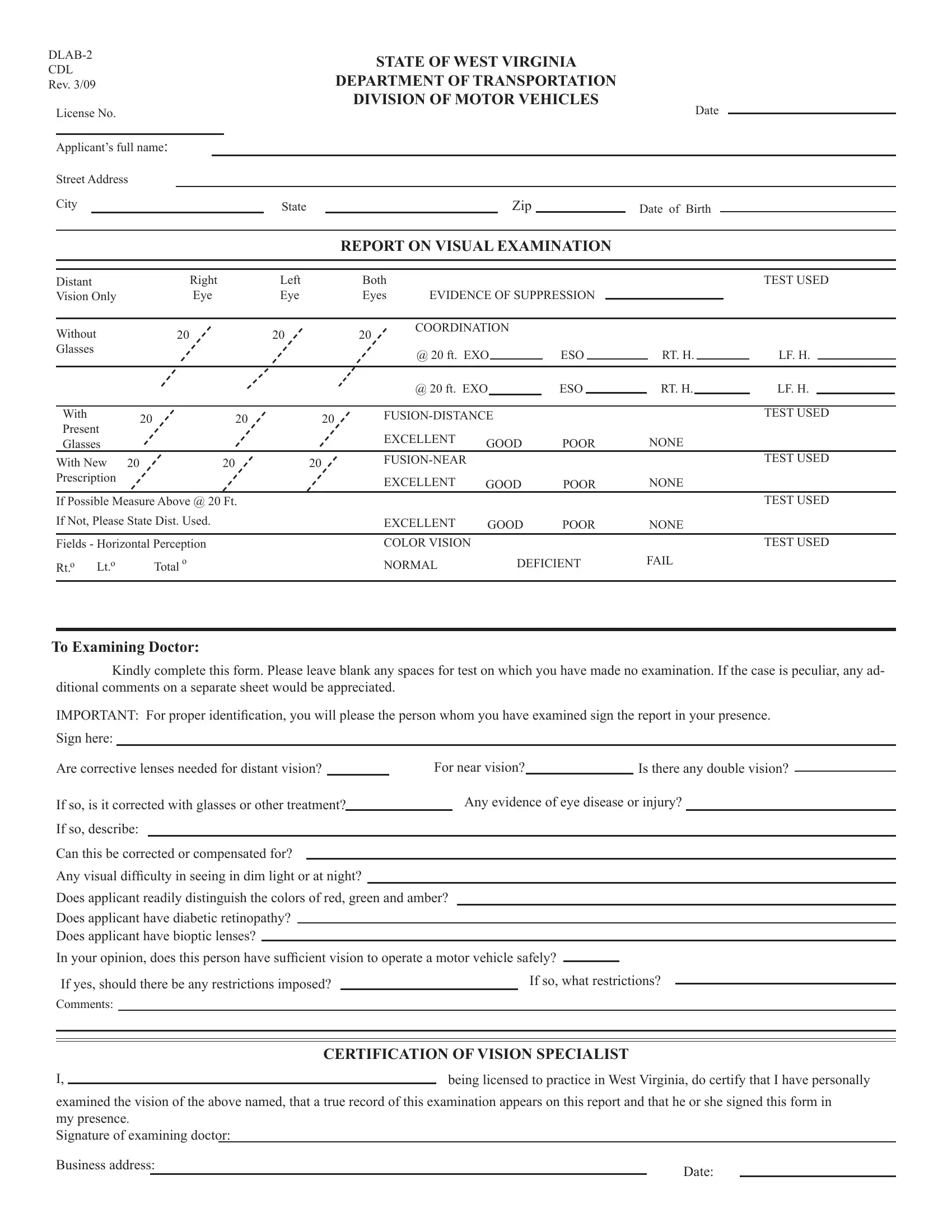
The DLAB-2 form, officially designated by the State of West Virginia's Department of Transportation, Division of Motor Vehicles, plays a crucial role in ensuring the safety of the roads and the well-being of those who navigate them. As a comprehensive assessment tool, it meticulously records the results of a visual examination required for commercial driver's license (CDL) applicants. Revised in March 2009, this document demands precise information, including the applicant's personal details and an extensive evaluation of their vision. Clear sections within the form allow for the detailed reporting of distant vision clarity, the presence of suppression, eye coordination, and fusion at various distances, both with and without corrective lenses. Additionally, it assesses the applicant's color vision, horizontal field perception, and any potential difficulties with night vision or the presence of eye diseases. The importance of accurate completion by a certified vision specialist cannot be overstated, as it includes a certification section where the examiner attests to the veracity of the information provided. This form not only determines the current visual capabilities of CDL applicants but also considers whether any restrictions should be recommended to ensure their safe driving. The DLAB-2 form, thus, stands as a testament to the commitment to road safety and the rigorous standards set for commercial drivers in West Virginia.
| Question | Answer |
|---|---|
| Form Name | Form Dlab 2 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | DLAB 2 CDL_Visual Examiniation Report_WEB wv dlab2 form |
|
|
|
|
|
|
|
|
STATE OF WEST VIRGINIA |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
CDL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
DEPARTMENT OF TRANSPORTATION |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Rev. 3/09 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
DIVISION OF MOTOR VEHICLES |
|
|
Date |
|
|
|
|
|||||||||||||
|
License No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Applicant’s full name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
State |
|
|
|
|
|
|
|
Zip |
|
|
|
|
|
Date of Birth |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
REPORT ON VISUAL EXAMINATION |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Distant |
|
|
Right |
Left |
|
|
Both |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TEST USED |
|||||
|
Vision Only |
|
|
Eye |
Eye |
|
|
Eyes |
EVIDENCE OF SUPPRESSION |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Without |
|
20 |
|
|
20 |
|
|
20 |
COORDINATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Glasses |
|
|
|
|
|
|
|
|
|
@ 20 ft. EXO |
|
|
|
ESO |
|
|
|
RT. H. |
|
|
|
|
LF. H. |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
@ 20 ft. EXO |
|
ESO |
|
|
RT. H. |
|
|
LF. H. |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
With |
20 |
20 |
|
20 |
|
|
|
|
|
|
|
|
|
|
|
TEST USED |
||||||||||||||
|
Present |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
EXCELLENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Glasses |
|
|
|
|
|
|
|
|
GOOD |
POOR |
|
NONE |
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
With New 20 |
|
20 |
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TEST USED |
||||||||
|
Prescription |
|
|
|
|
|
|
|
|
EXCELLENT |
GOOD |
POOR |
|
NONE |
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
If Possible Measure Above @ 20 Ft. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TEST USED |
||||||||
|
If Not, Please State Dist. Used. |
|
|
|
EXCELLENT |
GOOD |
POOR |
|
NONE |
|
|
|
|
||||||||||||||||||
|
Fields - Horizontal Perception |
|
|
|
COLOR VISION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TEST USED |
|||||||||
|
Rt.o Lt.o |
|
Total o |
|
|
|
NORMAL |
|
|
|
DEFICIENT |
FAIL |
|
|
|
|
|||||||||||||||
To Examining Doctor:
Kindly complete this form. Please leave blank any spaces for test on which you have made no examination. If the case is peculiar, any ad- ditional comments on a separate sheet would be appreciated.
IMPORTANT: For proper identification, you will please the person whom you have examined sign the report in your presence.
Sign here:
Are corrective lenses needed for distant vision? |
|
For near vision? |
|
Is there any double vision? |
|
||||
|
|
||||||||
If so, is it corrected with glasses or other treatment? |
|
Any evidence of eye disease or injury? |
|||||||
If so, describe: |
|
|
|
|
|
|
|
|
|
Can this be corrected or compensated for?
Any visual difficulty in seeing in dim light or at night?
Does applicant readily distinguish the colors of red, green and amber?
Does applicant have diabetic retinopathy?
Does applicant have bioptic lenses?
In your opinion, does this person have sufficient vision to operate a motor vehicle safely?
If yes, should there be any restrictions imposed? |
|
If so, what restrictions? |
|
|
|
|
|||
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CERTIFICATION OF VISION SPECIALIST |
|
I, |
|
being licensed to practice in West Virginia, do certify that I have personally |
|
||
examined the vision of the above named, that a true record of this examination appears on this report and that he or she signed this form in
my presence.
Signature of examining doctor:
Business address: |
Date: |
|