

Using PDF files online can be super easy using our PDF tool. You can fill in Form Dlse 666 here effortlessly. The editor is continually updated by our team, receiving handy features and turning out to be better. It merely requires a couple of easy steps:
Step 1: First, open the pdf editor by clicking the "Get Form Button" in the top section of this site.
Step 2: As soon as you launch the tool, you'll notice the document made ready to be completed. Apart from filling out various fields, you can also do various other things with the file, namely adding any words, editing the initial textual content, inserting graphics, placing your signature to the form, and much more.
Filling out this PDF will require thoroughness. Make sure that all necessary areas are filled in properly.
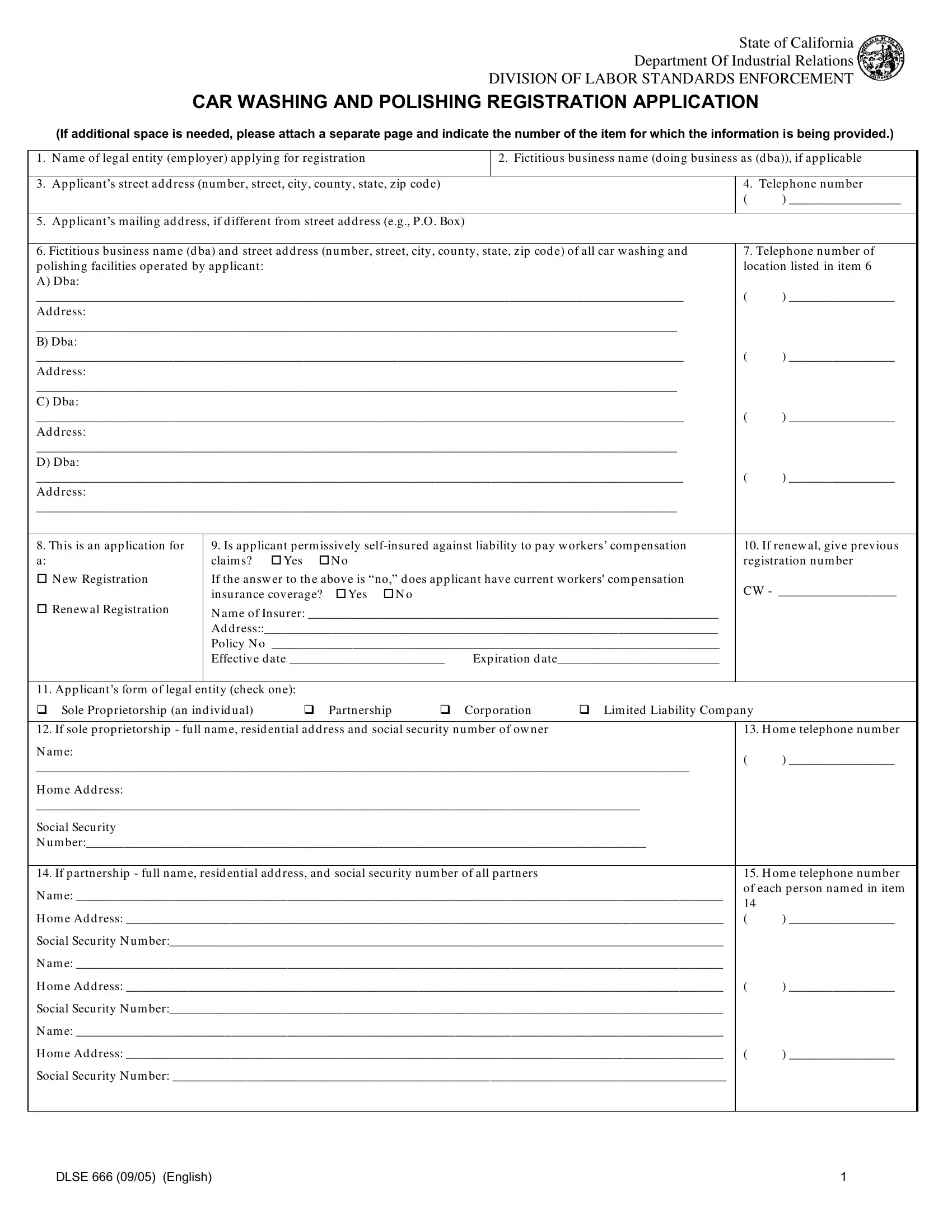
1. To get started, once filling out the Form Dlse 666, start out with the part that contains the next blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - This is an ap p lication for a N, Is ap p licant p erm issively, N am e of Insu rer Ad d ress, If renew al give p reviou s, Applicants form of legal entity, If sole p rop rietorship fu ll, N am e, H om e telep hone nu m ber, H om e Ad d ress, Social Secu rity N u m ber If p, N am e, H om e Ad d ress, Social Secu rity N u m ber, N am e, and H om e Ad d ress with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. This next segment is about Social Secu rity N u m ber, and DLSE English - complete each one of these blank fields.

4. Your next section will require your input in the following parts: If corp oration or LLC fu ll nam, m em bers, N am e and title, H om e Ad d ress, Social Secu rity N u m ber, N am e and title, H om e Ad d ress, Social Secu rity N u m ber, N am e and title, H om e Ad d ress, Social Secu rity N u m ber, Fu ll nam e resid ential ad d, management responsibility over any, N am e, and H om e Ad d ress. Ensure you provide all needed info to move further.
5. The very last section to conclude this document is crucial. Be certain to fill out the required blanks, like Social Secu rity N u m ber, N am e, H om e Ad d ress, Social Secu rity N u m ber, Fu ll nam e resid ential ad d, A N am e, H om e Ad d ress, Social Secu rity N u m ber, B N am e, H om e Ad d ress, Social Secu rity N u m ber, C N am e, H om e Ad d ress, Social Secu rity N u m ber, and D N am e, prior to submitting. In any other case, it could generate an incomplete and potentially invalid document!
As to D N am e and H om e Ad d ress, be certain you get them right in this current part. Those two are the key fields in this form.
Step 3: Just after rereading the entries, hit "Done" and you're all set! Go for a free trial account at FormsPal and get immediate access to Form Dlse 666 - download or edit inside your FormsPal account page. FormsPal offers risk-free document editor devoid of data recording or sharing. Rest assured that your data is in good hands here!